Abstract
We report a 54‑year‑old woman with chronic pancreatitis, duodenal obstruction, massive ascites, and refractory thrombocytopenia who developed septic obstructive cholangitis after occlusion of a plastic common bile duct (CBD) stent. Endoscopic exchange failed and PTBD was prohibitively risky. Transjugular intrahepatic biliary stenting (TIBS) provides an alternative route that avoids transperitoneal hepatic capsule puncture. Via right internal jugular access, the right hepatic vein was catheterized, a posterior sectoral bile duct punctured, and a guidewire crossed the distal CBD stricture. A 12 × 80 mm self‑expandable metallic stent was deployed and the transhepatic tract embolized with coils. The patient experienced rapid clinical and biochemical recovery (bilirubin, 13.3 to 1.37 mg/dL) over 9 days postprocedure without any hemorrhagic complications. TIBS is a decisive, life‑saving alternative when standard routes are not possible.
-
Keywords: Intrahepatic bile ducts; Cholangitis; Obstructive jaundice; TIPSS; Stent
Introduction
Obstructive jaundice due to biliary stricture or blockage often requires urgent decompression to prevent cholangitis and liver failure. The standard approaches for biliary drainage are endoscopic retrograde stenting or PTBD. However, these conventional routes can be infeasible or high-risk in certain situations. Massive ascites and coagulopathy (severe thrombocytopenia or coagulopathy) are relative contraindications to percutaneous transhepatic biliary interventions due to the high risk of hemorrhage and bile leakage into the peritoneum [
1]. In such high-risk cases—for example, when endoscopic access is blocked by duodenal obstruction or when coagulopathy cannot be corrected—an alternative route for biliary drainage is needed. A transjugular intrahepatic approach offers a viable alternative in these scenarios [
1]. This technique involves accessing the biliary system through the internal jugular vein and hepatic veins, thereby avoiding puncture of the liver capsule from the peritoneal side. We present a case of successful transjugular intrahepatic biliary stenting (TIBS) in a patient with distal biliary obstruction, refractory coagulopathy, and ascites. A comprehensive review of the literature is also provided to contextualize this approach, its indications, technique, and outcomes.
Case Report
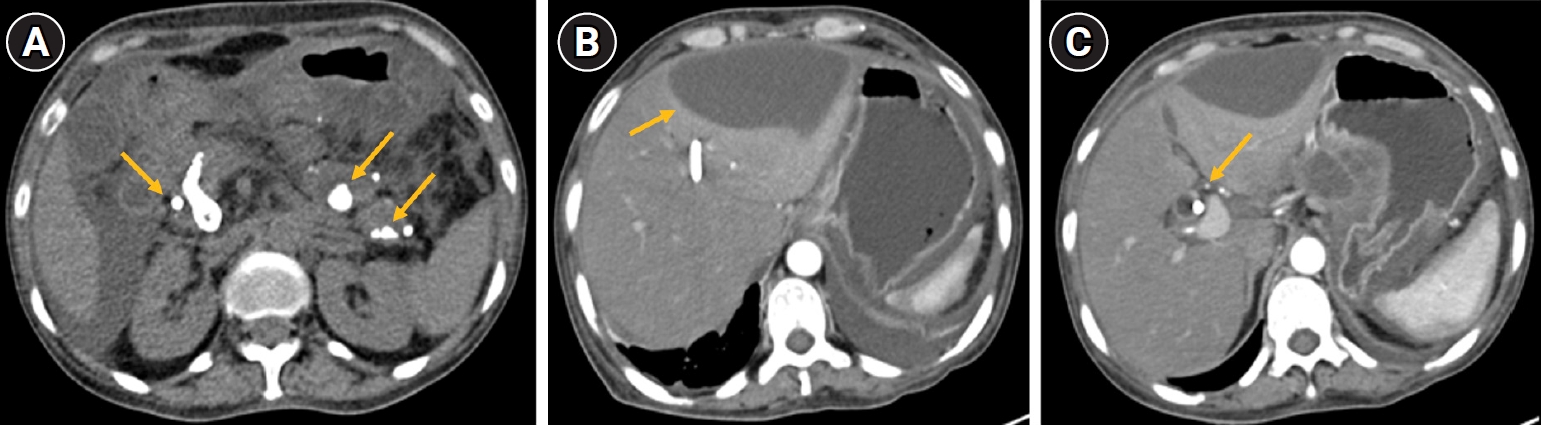
A 54-year-old woman presented with 15 days of progressive jaundice (yellowish discoloration of the eyes), intense pruritus, and upper abdominal pain. Her medical history was notable for chronic calcific pancreatitis with pancreatic ductal calculi and a distal common bile duct (CBD) stricture seen on a prior magnetic resonance cholangiopancreatography. She had undergone endoscopic plastic biliary stenting for the CBD stricture a few weeks earlier and an attempted pancreatic duct stenting had been unsuccessful. On current admission, she was markedly icteric and had signs of cholestatic liver dysfunction. A multiphasic contrast-enhanced computed tomography scan showed changes of chronic pancreatitis with extensive intraductal pancreatic calcifications. There were fluid collections in the lesser sac and anterior to the left liver lobe, along with moderate ascites (
Fig. 1). The previously placed biliary stent appeared to be occluded, with a significantly dilated biliary tree upstream. Notably, a small enhancing lesion in the head of the pancreas raised suspicion for pancreatic malignancy.
During the hospital course, the patient’s condition deteriorated: she developed acute cholangitis with high fever and septic shock requiring intensive care unit admission and vasopressor support. An attempt at endoscopic biliary stent exchange was made, but it failed due to a tight duodenal stricture with deep ulceration in the duodenum that prevented endoscope passage to the papilla. With the endoscopic route not possible, percutaneous transhepatic access was considered next. However, the patient had profound thrombocytopenia (platelet count 7,000/mm3, rising only to 12,000/mm3, after two single-donor platelet transfusions) and evidence of consumptive coagulopathy (elevated immature platelet fraction ~30%, peripheral smear showing low platelets with megakaryocytes, consistent with low-grade disseminated intravascular coagulation). Her prothrombin time was mildly prolonged (international normalized ratio, 1.38). Given the uncorrectable coagulopathy and presence of ascites, standard PTBD was deemed exceedingly high-risk for uncontrollable bleeding. After multidisciplinary discussion, a transjugular intrahepatic route was selected for biliary decompression as a last resort.
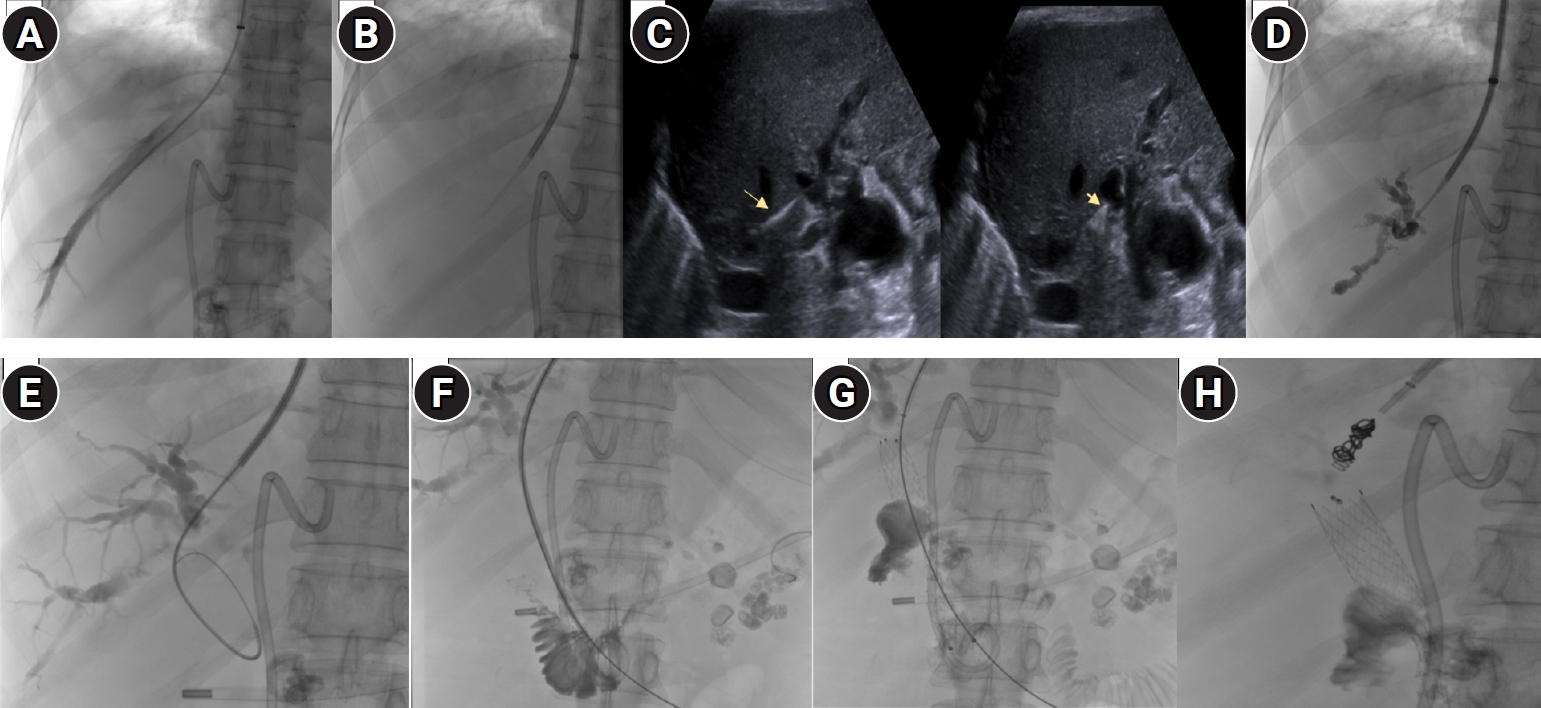
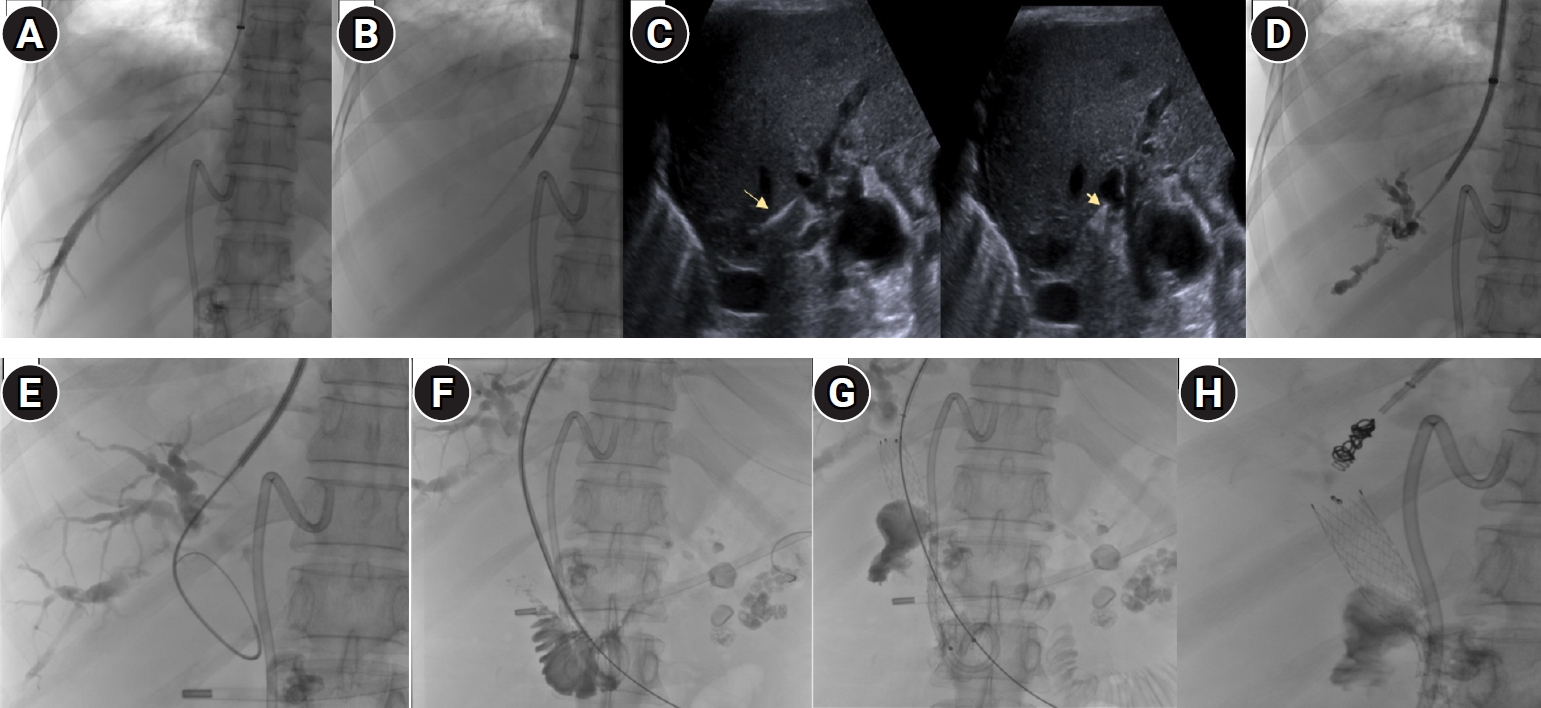
The procedure was performed in the interventional radiology suite under fluoroscopic guidance. A 10-Fr access in the right internal jugular vein was taken and a 5-Fr Multipurpose catheter was advanced into the right hepatic vein (RHV). Over an Ultra-stiff Amplatz wire the TIPS cannula was advanced (Cook Medical, Bloomington, IN, USA). Using ultrasound guidance provided by a second operator, the Colapinto needle was advanced to puncture the right biliary radicle from the RHV. The puncture technique was similar to a portal vein puncture while performing a TIPS procedure. Indentation of the bile duct was confirmed on ultrasonography, following which the puncture was made (
Video 1). Contrast was injected to confirm entry into the biliary tree with opacification of dilated intrahepatic ducts. A 0.035-inch Terumo guidewire along with a 4F Cobra (C1) glide-catheter (Terumo Corp., Tokyo, Japan) was used to negotiate through the obstructed bile duct. The stricture at the lower end of the CBD was successfully traversed, and the wire was advanced into the duodenum. The wire was exchanged for an Ultra-stiff Amplatz over which, a 12 × 80 mm self-expandable metallic stent (Luminexx, BD/BARD, Tempe, AZ, USA) was deployed across the distal CBD stricture, spanning from the proximal biliary tree into the duodenum. Free flow of contrast into the duodenum confirmed adequate decompression of the biliary system. Finally, to prevent hemorrhage or bile leak along the needle tract, the transhepatic tract between the RHV and the biliary duct was embolized. Two pushable coils measuring 35-5-3 mm and 35-14-4 mm (Cook Medical) were placed in the tract to seal it. The internal jugular access was then removed and hemostasis achieved (
Fig. 2).
Following the transjugular stent placement, the patient’s condition improved markedly. Her jaundice and fever subsided over the next few days as cholangitis resolved. Liver function tests showed rapid improvement: total bilirubin decreased from 13.3 mg/dL pre-procedure to 1.37 mg/dL at discharge. She was monitored in the hospital for 9 days post-procedure, during which no procedure-related complications (such as bleeding or hemobilia) occurred. The patient was discharged in stable condition with instructions for outpatient follow-up. At a 1-month follow-up, she remained clinically improved with the biliary stent functioning and no recurrence of biliary obstruction symptoms.
This case was conducted in accordance with the Declaration of Helsinki. As a retrospective observational report involving anonymized clinical data, formal ethics committee approval was not required at our institution; however, institutional review board exemption was confirmed. Patient confidentiality has been maintained throughout. Written informed consent was obtained from the patient for the publication of this case and any accompanying images.
Discussion
This case highlights the role of TIBS as a salvage technique when conventional methods are contraindicated or have failed. The presence of severe coagulopathy and ascites in our patient made percutaneous transhepatic access extremely dangerous, as puncturing the liver capsule under these conditions carries a high risk of intraperitoneal hemorrhage and bile peritonitis [
2]. Even with techniques like prior ascites drainage and tract embolization, PTBD in coagulopathic patients has a significantly elevated complication risk. The transjugular approach, first described in 1967 by Hanafee and Weiner. [
3] for cholangiography, avoids traversing the peritoneal cavity by accessing the biliary system via the hepatic veins. In essence, the needle puncture is entirely intrahepatic and any bleeding that occurs is more likely to be contained within the vascular system or tract, rather than filling the abdominal cavity. This approach was further developed in the 1990s, with early reports demonstrating transjugular insertion of biliary stents in patients with malignant obstructions complicated by ascites. Ring et al. reported the first use of an expandable metal stent via the transjugular route to palliate malignant biliary obstruction in a patient with refractory ascites [
4]. Subsequent case reports, including the study by Amygdalos et al. in 1996 [
1], reinforced that transjugular biliary catheterization is a valuable alternative when standard PTBD is contraindicated.
The TIBS requires advanced skill and careful technique. Under imaging guidance, a hepatic vein (usually RHV) is catheterized from the internal jugular route. A Colapinto or Rösch needle is used to puncture from the hepatic vein through a small portion of liver parenchyma into an intrahepatic bile duct [
2]. Key technical steps include choosing a peripheral biliary branch to puncture (to minimize the tract size and bleeding risk) and using real-time ultrasound guidance to aid the needle puncture. Once access to a dilated bile duct is confirmed by cholangiography, a guidewire and catheter are advanced across the biliary obstruction. In our case and others, a hydrophilic guidewire can be maneuvered through a distal CBD stricture into the duodenum. If the guidewire successfully crosses the obstruction, the tract can be dilated to allow passage of catheters and eventually a stent. Self-expandable metal stents (uncovered or covered) of adequate length are then deployed across the stricture to re-establish biliary drainage into the gastrointestinal tract. A completion cholangiogram or radiograph is performed to ensure contrast flows freely past the stent into the duodenum or bowel, confirming patency. Finally, an important step—especially in coagulopathic patients—is embolization of the created tract. After stent placement, the needle tract through the liver is occluded using coils to prevent any bleeding leading to hemobilia. In the presented case, coils were used; some protocols use N-butyl cyanoacrylate (glue) mixed with lipiodol for tract sealing [
5]. Tract embolization has been shown to reduce post-procedure hemorrhage and bile leak complications in both percutaneous and transvenous approaches.
Our patient’s successful outcome aligns with the growing body of evidence supporting transjugular biliary interventions in high-risk patients. While no large randomized trials exist (owing to the relatively infrequent use of this technique), multiple small studies and case reports have documented its feasibility. A prospective study of 12 patients by Shim et al. (2019) [
2] is one of the largest studies to date evaluating TIBS in malignant obstructions with massive ascites/coagulopathy. Technical success of 92% and clinical success of 73% was reported. The main complication noted in that study was hemobilia in two patients. Notably, all patients had advanced malignancy, and the median overall survival was only 19 days due to disease progression—emphasizing that TIBS in such contexts is often a palliative measure to improve quality of life in end-stage patients.
Another notable study by Tsauo et al. [
5] reported on six patients with distal malignant biliary obstruction and uncorrectable coagulopathy who underwent transjugular bare-metal stent insertion. The authors concluded that when the risk of hemorrhage from percutaneous drainage is prohibitively high, TIBS is an effective alternative for palliation of obstructive jaundice. They reported an average survival of 4.5 months in their study, with 100% stent patency until death. This suggests that once the immediate hurdle of safely establishing drainage is overcome, TIBS can sustain biliary decompression adequately. Our case reinforces this conclusion, demonstrating that TIBS can be life-saving in the setting of disseminated intravascular coagulation and thrombocytopenia where PTBD is essentially impossible.
It is also valuable to compare the transjugular approach to the modified percutaneous strategies developed for patients with ascites. Seif et al. [
6] described a “one-stage percutaneous triple procedure” for malignant biliary obstruction with marked ascites, which involves large-volume paracentesis (ascites drainage), immediate placement of a biliary metal stent, and then embolization of the tract with glue, all in one session. In a study of 25 patients treated with this method, technical success was 96% and major complications were avoided by prophylactically sealing the tract. While that approach is highly effective when ascites is the main issue, it still requires that coagulation parameters be reasonably controlled; bleeding can still occur if platelets or clotting factors are critically low. TIBS is technically demanding and not as widely practiced as standard PTBD or endoscopic stenting. The success of the procedure hinges on being able to target a suitable bile duct from the venous side. Failure can occur if the bile ducts are small or not sufficiently dilated to be located, or if the stricture cannot be crossed with a guidewire.
Meticulous tract management is paramount during and after hepatic interventions: coil embolization under ultrasound guidance should be performed to prevent bile-venous communications. The rationale is hemodynamic—a higher pressure in the CBD (approximately 12–14 mmHg) relative to the hepatic vein (around 7 mmHg) can drive bile directly into the hepatic venous system. Clinically, this manifests as bilhemia, marked by a rapid rise in total and direct bilirubin without other evidence of hepatic dysfunction or biliary obstruction. It most often follows hepatic trauma but has also been observed after TIPS. This mechanism differs from portal venous–biliary fistulas, in which the higher-pressure portal circulation delivers blood into the biliary tree, resulting in hemobilia [
7-
9].
Our patient’s recovery from multi-organ dysfunction after biliary decompression illustrates how critical timely drainage is, and TIBS provided a means to achieve it when no other safe option was available.
TIBS is an important alternative technique for biliary drainage in patients who have contraindications to the standard endoscopic or percutaneous approaches. In the presence of uncorrectable coagulopathy, severe thrombocytopenia, or massive ascites, the transjugular approach can be life-saving, allowing relief of biliary obstruction with a lower risk of catastrophic bleeding. The literature, though composed of case studies and reports, consistently demonstrates that TIBS is technically feasible and clinically effective in achieving jaundice relief in high-risk patients. The case presented here adds to this body of evidence, showing successful application of TIBS in a scenario of disseminated intravascular coagulation and duodenal obstruction. While TIBS requires specialized expertise and may not be available in all centers, it should be considered in the armamentarium for complex biliary obstruction cases. Transjugular route offers a robust solution to achieve biliary decompression and resolve obstructive cholangitis, ultimately improving patient outcomes in otherwise dire circumstances.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Acknowledgments
None.
Author contributions
Conceptualization: SS, HR, AK, SSB. Writing – original draft: SS. Writing – review & editing: SS, SSB.
Data availability statement
Data sharing does not apply to this article as no datasets were generated or analyzed during the current study.
Supplementary material
Fig. 1.Intraductal calculi (depicted by arrows) in the head, body, and tail region of pancreas (A), fluid collection (arrow) along the anterior aspect of the left lobe of the liver (B), and a common bile duct (CBD) stent (arrow) with dilated CBD and pseudocyst in the lesser sac and a fluid collection along the anterior aspect of the left lobe of liver (C).
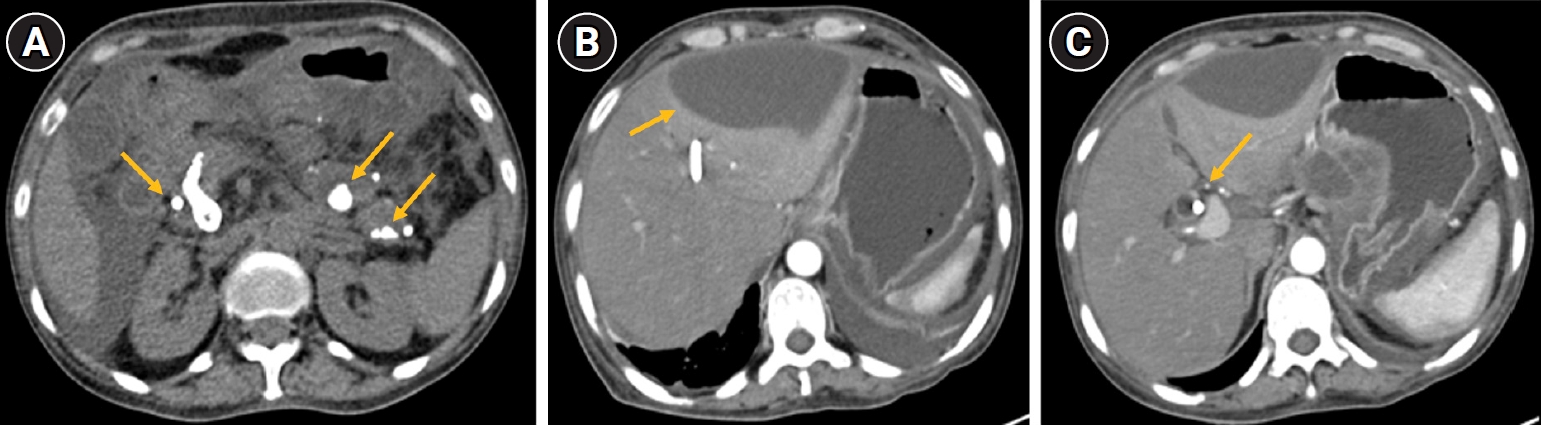
Fig. 2.(A) Right hepatic vein venography. (B) Transjugular liver biopsy (Cook Medical) set cannula through which a Rosch Uchida TIPS set (RUPS set, Cook Medical) catheter stylet combination advanced to puncture the right posterior sectoral duct (RPSD). (C) Ultrasonography guidance demonstrates sludge within dilated biliary ducts (arrowhead) and puncture of the RPSD (arrow). (D) Cholangiography. (E) A 0.035-inch angled glidewire (Terumo Corp.) negotiated into the common bile duct (CBD). (F) A 4-Fr catheter used to assist in negotiating the guidewire across the stricture into the duodenum. (G) Metallic stent deployed across the stricture. (H) The intrahepatic veno-biliary track embolized with pushable coils.
References
- 1. Amygdalos MA, Haskal ZJ, Cope C, Kadish SL, Long WB. Transjugular insertion of biliary stents (TIBS) in two patients with malignant obstruction, ascites, and coagulopathy. Cardiovasc Intervent Radiol. 1996;19:107-109. https://doi.org/10.1007/BF02563903
- 2. Shim DJ, Gwon DI, Ko GY, Yoon HK, Sung KB. Transjugular insertion of biliary stent in patients with malignant biliary obstruction complicated by ascites with/without coagulopathy: a prospective study of 12 patients. Diagn Interv Radiol. 2019;25:465-470. https://doi.org/10.5152/dir.2019.18470
- 3. Hanafee W, Weiner M. Transjugular percutaneous cholangiography. Radiology. 1967;88:35-39. https://doi.org/10.1148/88.1.35
- 4. Ring EJ, Gordon RL, LaBerge JM, Shapiro HA. Malignant biliary obstruction complicated by ascites: transjugular insertion of an expandable metallic endoprosthesis. Radiology. 1991;180:579-581. https://doi.org/10.1148/radiology.180.2.2068334
- 5. Tsauo J, Li X, Li H, Wei B, Luo X, Zhang C, et al. Transjugular insertion of bare-metal biliary stent for the treatment of distal malignant obstructive jaundice complicated by coagulopathy. Cardiovasc Intervent Radiol. 2013;36:521-525. https://doi.org/10.1007/s00270-012-0453-6
- 6. Seif HM, Zidan M, Helmy A. One-stage percutaneous triple procedure for treatment of endoscopically unmanageable patients with malignant biliary obstruction and marked ascites. Arab J Gastroenterol. 2013;14:148-153. https://doi.org/10.1016/j.ajg.2013.10.004
- 7. Kruel CR, Guimaraes M, Chedid AD, Grezzana-Filho TM, Leipnitz I, Araujo Ad, et al. Bilhemia following transjugular intrahepatic portosystemic shunt placement (TIPS): liver transplantation as a rescue procedure - case report. Arq Bras Cir Dig. 2013;26:238-240. https://doi.org/10.1590/s0102-67202013000300016
- 8. Blum U, Buitrago-Tellez C, el Seif M, Wimmer B. Posttraumatic bilhemia: conservative management by percutaneous drainage. Cardiovasc Intervent Radiol. 1993;16:55-57. https://doi.org/10.1007/BF02603040
- 9. Singal AK, Kathuria MK, Malhotra A, Goodgame RW, Soloway RD. Bilhemia after trans-jugular intra-hepatic porto-systemic shunt and its management with biliary decompression. World J Gastroenterol. 2009;15:3681-3683. https://doi.org/10.3748/wjg.15.3681