Abstract
Chronic limb-threatening ischemia represents the most severe form of peripheral artery disease and is associated with high risks of limb loss and mortality. It is closely associated with below-the-knee arterial disease, with substantial overlap between the two conditions, particularly in patients with diabetes. Endovascular treatment plays a central role in restoring distal tibial and pedal perfusion, which is critical for wound healing and limb salvage. However, it remains technically challenging due to small vessel size, diffuse disease, and heavy calcification, which limit luminal expansion and predispose to recoil, dissection, and restenosis. Procedural success requires a structured approach integrating access strategy, guidewire crossing, and subsequent treatment. Crossing strategies, including subintimal tracking, retrograde tibio-pedal access, and bidirectional techniques such as controlled antegrade and retrograde tracking, are often required in complex lesions. Plain balloon angioplasty remains the most broadly applicable treatment, whereas drug-coated balloons show inconsistent benefit. Drug-eluting stents provide favorable outcomes in selected short focal lesions, whereas other technologies have more limited evidence. Overall, treatment should be individualized based on lesion characteristics and clinical context.
-
Keywords: Peripheral artery disease; Chronic limb-threatening ischemia; Below-the-knee; Endovascular treatment
Introduction
Below-the-knee (BTK) arterial disease should be understood within the broader epidemiologic context of peripheral artery disease (PAD). PAD affects approximately 12% to 14% of the general population, increases markedly with age, and has grown substantially worldwide, from 164 million people in 2000 to 202 million in 2010 [
1,
2]. This expanding and aging PAD population represents a major driver of the increasing global burden of advanced limb ischemia.
Chronic limb-threatening ischemia (CLTI) represents the most severe clinical subset of PAD. The 2024 American College of Cardiology/American Heart Association guidelines for lower-extremity PAD identify CLTI as one of the major clinical presentations of PAD and frame it as a limb-threatening condition requiring timely evaluation and treatment [
3]. Epidemiologically, CLTI represents a substantial disease burden, with an estimated prevalence of approximately 6.5 million individuals across the United States, Europe, and Japan, and is associated with a 1-year mortality of about 20%–25% and a 5-year all-cause mortality exceeding 50% [
4-
6]. Clinically, CLTI presents with rest pain, non-healing wound, or gangrene, and reflects not only arterial obstruction itself but also the combined burden of impaired perfusion, tissue loss, infection risk, and systemic frailty.
Importantly, CLTI and BTK disease overlap to a very large extent. BTK disease has been reported in more than 70% of patients with CLTI, particularly among patients with diabetes [
6]. In addition, approximately one-third of patients with critical limb ischemia present with isolated BTK lesions, which have been associated with a higher incidence of limb loss than multilevel disease [
7]. Accordingly, restoration of distal tibial and pedal perfusion is a critical determinant of wound healing and limb salvage in patients with CLTI. Treatment of more proximal disease alone is insufficient when distal runoff remains severely compromised [
6,
8].
This close relationship between CLTI and BTK disease explains why endovascular revascularization has a central role in contemporary management. The therapeutic goal is not simply angiographic patency, but restoration of perfusion sufficient to relieve ischemic pain, promote wound healing, and prevent major amputation [
8]. Current guidelines consistently position revascularization as a key treatment component in CLTI management [
3,
9]. The 2024 European Society of Cardiology (ESC) Guidelines for the management of peripheral arterial and aortic diseases recommend revascularization as soon as possible in CLTI and state that endovascular revascularization is the treatment of choice for short BTK lesions [
9].
Pathophysiology
BTK PAD differs from more proximal lower-extremity disease not only in lesion distribution but also in arterial structure and biomechanics. Compared with femoropopliteal arteries, BTK arteries are smaller, thinner, more frequently calcified, and mechanically stiffer in the longitudinal direction, with distinct structural composition including lower elastin, collagen, and glycosaminoglycan content [
10].
The distribution and morphology of calcification also differ along the lower-extremity arterial tree. As the arterial tree progresses distally toward the tibial vessels, calcified plaques increase while fibrofatty plaques decrease, reflecting a progressive shift in plaque composition [
6]. In BTK arteries, calcification is not only more prevalent but also a key determinant of vessel behavior, as it directly affects arterial compliance and response to endovascular treatment.
In particular, calcification in BTK arteries may involve both the intimal and medial layers, which have distinct biological and mechanical implications [
11,
12]. Intimal calcification is typically associated with atherosclerotic plaque and contributes directly to luminal narrowing, whereas medial calcification is more closely linked to systemic metabolic disease, particularly diabetes mellitus and chronic kidney disease, and results primarily in circumferential stiffening and loss of arterial compliance [
12,
13]. In a histopathologic study of lower-extremity arteries, hemodialysis was identified as an important factor associated with severe medial calcification in BTK lesions, whereas diabetes was not independently associated with severe medial calcification after multivariable adjustment [
12].
These structural and pathologic differences have direct procedural implications. Compared with femoropopliteal arteries, BTK intervention is more vulnerable to limited luminal gain, elastic recoil, dissection, and restenosis [
10,
14]. In heavily calcified BTK arteries, particularly when circumferential calcification predominates, balloon angioplasty may produce limited luminal expansion despite successful wire crossing because the artery behaves as a rigid, poorly compliant tube rather than a readily expandable stenotic plaque. This often results in substantial residual stenosis or elastic recoil. In contrast, more focal or eccentric calcification may predispose the vessel to flow-limiting dissection during balloon expansion [
11,
13]. Accordingly, the morphologic pattern of calcification, rather than its mere presence, directly influences endovascular strategy. This provides a mechanistic basis for the growing use of lesion-modifying techniques such as specialty balloons, atherectomy, or intravascular lithotripsy when conventional angioplasty alone is unlikely to achieve adequate expansion, although their clinical benefit remains uncertain [
11,
13,
15].
Technical Considerations in BTK Intervention
Target Vessel Selection
In CLTI with tissue loss, target vessel selection should first aim to establish in-line flow to the foot through at least one patent tibial artery [
3,
9]. Beyond this general principle, the angiosome concept may guide selection of the wound-related artery [
3,
8,
9]. Direct revascularization of the artery supplying the wound territory is generally preferred when technically feasible, whereas indirect revascularization through collateral networks may be acceptable when direct targeting is not feasible [
3,
8]. Lesion anatomy, vessel quality, collateral networks, pedal arch integrity, and technical feasibility should also be considered when selecting the target vessel.
In BTK intervention, antegrade femoral access is generally preferred when there is no significant disease in the common femoral artery or at the ostium of the superficial femoral artery. As lesions become longer, more calcified, and more distal, wire control and torque transmission become increasingly important. Antegrade access shortens the working distance and improves support, pushability, and particularly torquability of the guidewire and devices during tibial and pedal interventions. Consistent with this concept, advancement of the sheath as distally as feasible, often to the popliteal segment, has been recommended to further improve device support and control during BTK procedures [
16].
Crossing strategy in BTK chronic total occlusion (CTO) is largely lesion dependent. The Japanese BTK CTO score is useful because it translates angiographic morphology into practical crossing difficulty and predicts the likelihood of successful antegrade guidewire passage. In the original derivation cohort, five adverse angiographic variables predicted unsuccessful crossing: blunt proximal stump, calcification at the proximal entry, reference vessel diameter <2.0 mm, CTO length ≥200 mm, and absence of distal outflow in the target vessel. Successful guidewire crossing decreased from 97.3% in grade A to 76.8% in grade B, 19.3% in grade C, and 0% in grade D lesions [
17]. Prospective validation confirmed similar directional performance, with successful antegrade crossing rates of 97.5%, 89.1%, 62.5%, and 27.3% across grades A through D, respectively [
18]. Although the score is not universally adopted in routine practice, it highlights a fundamental concept: complex BTK CTO morphology is a major predictor of failure of simple antegrade intraluminal navigation. In such situations, subintimal tracking, retrograde tibio-pedal access, or bidirectional approaches frequently become necessary components of the procedural strategy [
6,
15,
16,
19].
Retrograde tibial or pedal access is primarily used as a bailout strategy in complex BTK CTO intervention when antegrade crossing is unsuccessful [
15]. One theoretical advantage is that the distal cap of the occlusion is often softer and more penetrable than the proximal cap, which may facilitate guidewire entry from below [
6].
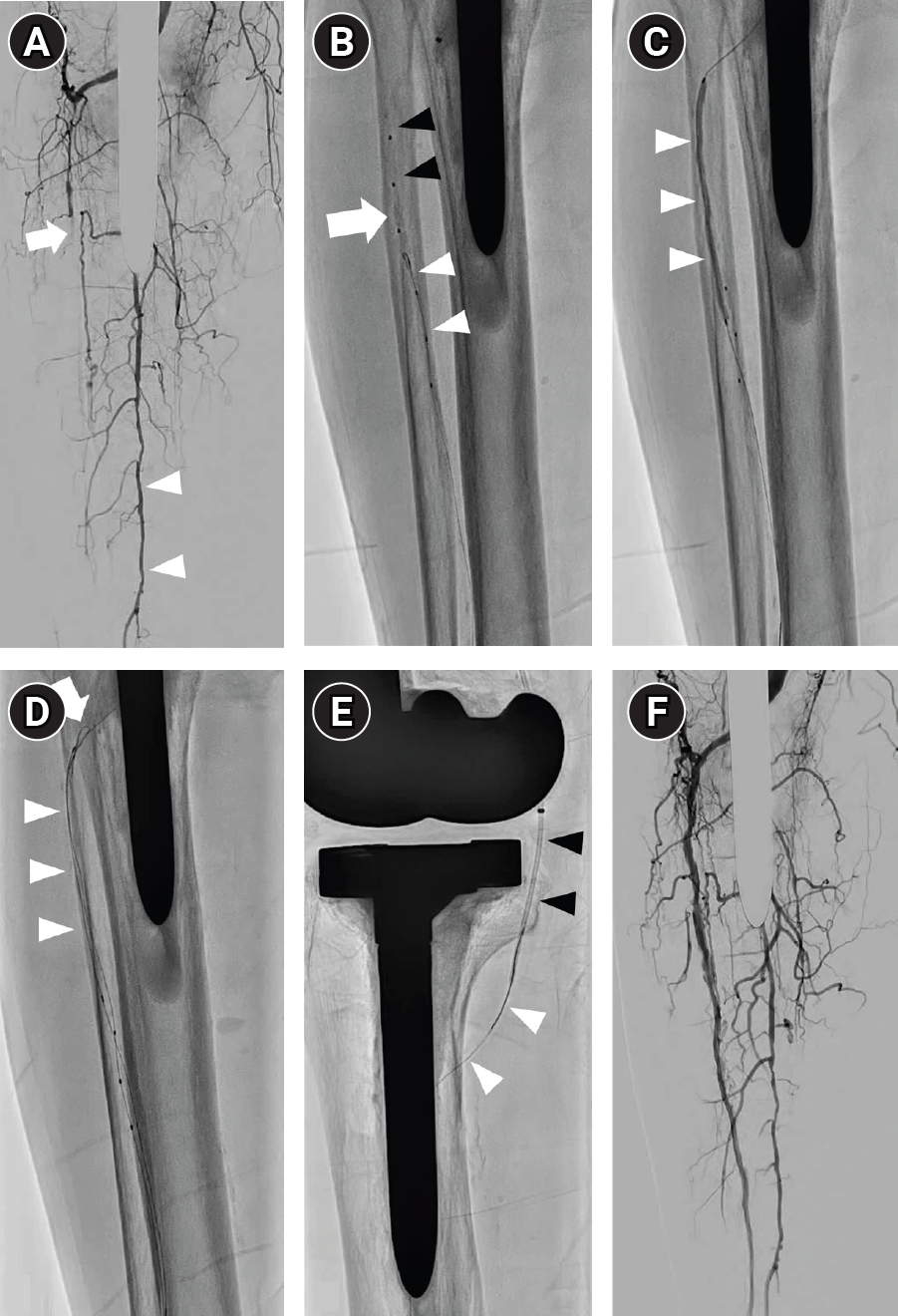
In addition, retrograde access is essential for conversion to a bidirectional strategy, such as controlled antegrade and retrograde subintimal tracking (CART) or reverse CART (
Fig. 1) [
6]. This technique is typically used when both antegrade and retrograde guidewire attempts fail to achieve true lumen re-entry, and the wires remain within separate subintimal spaces. A balloon is introduced from one direction to enlarge the subintimal space and create communication between the two channels. After balloon deflation, a guidewire in the opposite direction is advanced to enter the same subintimal plane and establish continuity between the antegrade and retrograde tracks. This bidirectional approach can substantially increase the likelihood of successful wire crossing when a single-directional wiring attempt fails.
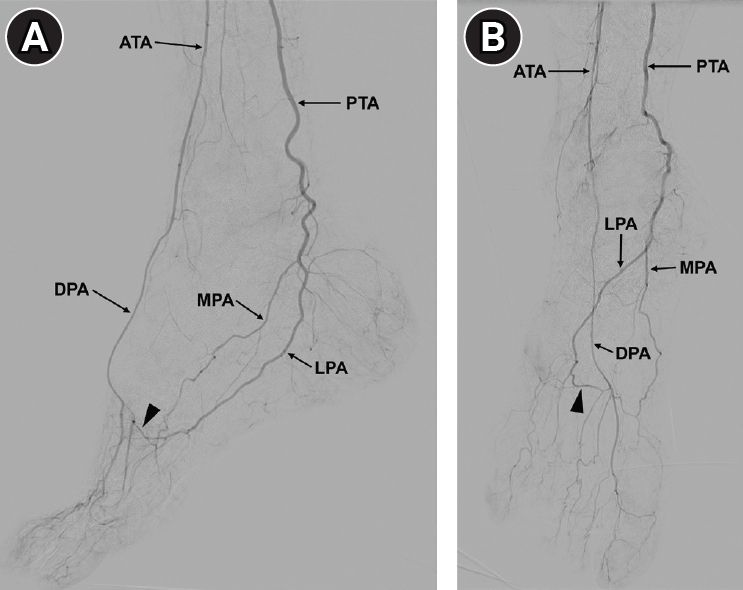
Anatomically, the pedal–plantar loop is formed by the dorsalis pedis artery, deep perforating artery, lateral plantar artery, and posterior tibial artery, providing potential collateral continuity between the anterior and posterior tibial circulations in the majority of individuals (
Fig. 2) [
16].
Pedal arch intervention should not be performed routinely and should be reserved for selected cases because of the relatively high risk of complications and restenosis [
6]. It becomes most relevant in wound-oriented revascularization when restoration of forefoot perfusion is required, particularly in patients with tissue loss involving the distal foot or multiple angiosomes [
6,
16]. Observational studies suggest that pedal arch patency is associated with improved wound healing, limb salvage, and survival in CLTI populations, particularly among patients with diabetes [
20,
21]. In addition, in selected cases, restoration of pedal arch continuity may improve distal runoff and thereby support the durability of BTK interventions, as inadequate distal outflow can promote thrombosis and restenosis in the treated segment.
The pedal arch may also serve as a conduit for trans-arch recanalization [
15]. A guidewire can be advanced across the pedal–plantar loop from the anterior tibial–dorsalis pedis system into the plantar and posterior tibial circulation, or in the opposite direction, thereby enabling retrograde crossing of tibial occlusions when direct retrograde pedal puncture is difficult.
Technical execution requires particular caution because pedal arch vessels are small in caliber and frequently tortuous [
6]. Navigation is typically performed using soft 0.014-inch guidewires together with low-profile microcatheters or balloons to minimize the risk of dissection injury. If pedal arch angioplasty is required, conservative balloon sizing is generally preferred in order to reduce the risk of rupture or flow-limiting dissection. Manipulation within the plantar circulation should also be minimized because excessive instrumentation can injure fragile distal vessels.
Failure of balloon passage after successful guidewire crossing is a common technical challenge in BTK intervention and is usually related to severe calcification, vessel tortuosity, or insufficient device support. In such situations, predilation with a low-profile single-marker balloon in the 1.2–1.5 mm range should be the first step [
22].
If balloon crossing remains unsuccessful, wire externalization using additional retrograde pedal access and creation of a through-and-through tensioned rail should be considered early. This configuration can substantially improve pushability and facilitate device delivery across resistant segments [
23,
24].
When these strategies fail, advanced plaque-modifying techniques may be considered as bailout options. Percutaneous direct needle puncture of calcified plaque (PIERCE) and its variants, including inner PIERCE, involve direct puncture of heavily calcified plaque using a needle to disrupt the calcification and facilitate subsequent device advancement [
25,
26]. Although these techniques can enable balloon delivery in otherwise uncrossable lesions, they carry risks such as perforation, dissection, or loss of collateral channels [
22]. Therefore, these advanced plaque-modifying techniques should be regarded as expert-level bailout maneuvers rather than routine procedural steps and should be reserved for patients with advanced diseases. The overall procedural workflow for BTK intervention is summarized in
Fig. 3.
Endovascular Treatment Strategies in BTK Disease
Plain Balloons vs. Drug-Coated Balloons
Percutaneous transluminal angioplasty (PTA), referring to plain balloon angioplasty without drug coating, remains the most commonly used treatment and continues to serve as a practical first-line approach in many settings, and the evidence comparing drug-coated balloons (DCB) with PTA in BTK disease remains inconsistent and does not demonstrate a clear clinical advantage. Positive signals have been reported in some single-center randomized trials. In the DEBATE-BTK trial, freedom from clinically driven target lesion revascularization (CD-TLR) at 1 year was 82% with DCB versus 63% with PTA (p = 0.002). However, by 5 years, differences in CD-TLR, major amputation, and all-cause mortality were no longer statistically significant [
27]. These findings are broadly consistent with those of a recent meta-analysis comparing DCB with PTA in CLTI patients, which found that DCB reduced CD-TLR at 12 months (OR, 0.39; 95% CI, 0.04 to 0.73). However, no significant differences were observed in major amputation, all-cause mortality, 6-month primary patency, or late lumen loss [
28]. These findings indicate that DCB may reduce early repeat revascularization but do not provide a sustained benefit in major clinical outcomes. In addition, the benefit of DCB in reducing early repeat revascularization has not been consistently demonstrated across the broader literature, including another meta-analysis or randomized trials [
15,
29-
33], and therefore does not support routine use of DCB in BTK artery disease.
Guideline recommendations reflect this uncertainty. The ESC guidelines state that drug-eluting balloons have not demonstrated superiority over PTA in BTK disease [
9]. In CLTI requiring BTK artery revascularization, contemporary guidelines emphasize timely revascularization and limb-salvage goals rather than prioritizing a specific device platform [
3,
9].
Unlike bare-metal stents (BMS), which demonstrate limited long-term patency in BTK arteries, drug-eluting stents (DES) provide both mechanical scaffolding and local delivery of antiproliferative agents, and represent one of the most studied implant-based therapies for BTK lesions. However, most of the available evidence is derived from studies involving selected patients with relatively short focal lesions [
34]. In the DESTINY trial, everolimus-eluting stents were compared with BMS in BTK lesions with a mean lesion length of 15.9 ± 10.2 mm [
35]. DES demonstrated significantly higher primary patency and lower target lesion revascularization (TLR) at 12 months. Similarly, the ACHILLES trial showed superiority of sirolimus-eluting stents over PTA in BTK lesions with a mean lesion length of 27 ± 21 mm [
36]. The DESTINY2 study assessed DES in slightly longer BTK lesions (mean lesion length, 47.4 ± 25 mm) and showed 12-month outcomes of 75.4% primary patency, 94.4% limb salvage, and 84.9% freedom from TLR [
37]. In addition, Giaquinta et al. [
38] reported outcomes of everolimus-eluting stents in BTK lesions with an average lesion length of 52.7 mm. Primary patency, limb salvage, and freedom from TLR were 88.9%, 93%, and 91.5% at 1 year, and 80.1%, 89.3%, and 85.1% at 3 years, respectively.
Taken together, the available evidence supports the use of DES primarily for selected short, focal BTK lesions. However, these results should be extrapolated with caution to the long, diffuse, and heavily calcified lesions commonly encountered in CLTI, as occlusion of the stented segment may complicate subsequent reintervention.
Bioresorbable Scaffolds
Bioresorbable scaffolds were developed to provide temporary mechanical support and drug delivery without leaving a permanent metallic implant in the tibial artery. The early experience was encouraging. In a pooled individual-patient analysis of 161 lesions in 121 patients treated with everolimus-eluting bioresorbable vascular scaffolds, freedom from restenosis was 91.7% at 12 months and 86.6% at 24 months, freedom from CD-TLR was 97.2% and 96.6%, and major amputation rate was 1.6% [
39]. The strongest randomized evidence now comes from the LIFE-BTK trial [
40]. In that multicenter trial, 261 CLTI patients were randomized 2:1 to a drug-eluting resorbable scaffold or PTA, and the mean lesion length was 44.1 ± 30.9 mm. At 2 years, the primary efficacy endpoint was achieved in 68.8% of the scaffold group compared with 45.4% in the PTA group (p < 0.001). Binary restenosis and CD-TLR were also significantly lower in the scaffold group, while the primary safety endpoint was similar between groups [
41]. Overall, although bioresorbable scaffolds have shown promising early outcomes and theoretical advantages over permanent metallic stents, the current evidence remains limited, and further studies are required to clarify their long-term efficacy and safety.
Atherectomy has an intuitively attractive role in BTK intervention because tibial lesions are frequently long, diffusely diseased, and heavily calcified, and conventional balloon angioplasty in this setting is often limited by inadequate luminal expansion, recoil, and dissection [
13]. In theory, plaque debulking or calcium modification before adjunctive balloon angioplasty could improve vessel compliance and reduce severe balloon-related vessel injury. However, despite this mechanistic appeal, the clinical evidence supporting atherectomy in BTK disease remains limited and inconsistent. Most available data are derived from small prospective series or retrospective observational studies, with only very limited randomized evidence and substantial heterogeneity in lesion characteristics across studies [
42,
43]. Importantly, the overall literature does not show a reproducible clinical advantage of atherectomy over balloon angioplasty alone in terms of procedural success, limb salvage, or freedom from TLR [
42]. In contrast, safety considerations can particularly be relevant because distal embolization from atherectomy in small-caliber tibial vessels with limited distal runoff may lead to significant harm in patients with CLTI, while distal embolic protection is not well established [
15,
44].
Taken together, the current evidence does not support the routine use of atherectomy for BTK disease. Atherectomy may be considered selectively in heavily calcified tibial lesions in which balloon expansion is expected to be inadequate, but its use should remain individualized, lesion-specific, and cautious. The treatment options for BTK intervention are summarized in
Table 1.
Conclusion
BTK intervention is a central component in the management of CLTI, but outcomes are constrained by the intrinsic characteristics of tibial arteries, including small vessel size, diffuse disease, and heavy calcification.
No single device strategy has demonstrated consistent superiority across the full spectrum of BTK disease. Balloon angioplasty remains the most broadly applicable approach, while DES show benefit in selected short focal lesions; other technologies, including bioresorbable scaffolds and plaque-modifying devices, have more limited and context-dependent evidence.
Ultimately, the key challenge is not simply achieving procedural success, but improving the durability of revascularization to sustain wound healing and limb preservation in a disease setting characterized by diffuse pathology and frequent restenosis.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Acknowledgments
The authors used ChatGPT for language editing. The authors take full responsibility for the content.
Author contributions
Conceptualization: TWC. Investigation: TWC, JHW, JK. Supervision: JHW, JK. Writing of the original draft: TWC. Writing of the review and editing: TWC, JHW, JK.
Data availability statement
No new data were generated or analyzed in this study. Data sharing is not applicable to this article.
Fig. 1.Reverse controlled antegrade and retrograde tracking technique for guidewire crossing. (A) Pre-procedural angiography demonstrates chronic total occlusion of the anterior tibial artery (arrow) and posterior tibial artery, with foot perfusion maintained only through collateral flow from the peroneal artery (arrowheads). (B) To cross a severely calcified chronic total occlusion of the anterior tibial artery (white arrow), antegrade (black arrowheads) and retrograde tracking via pedal puncture (white arrowheads) were attempted but ended in different subintimal spaces. (C) A balloon catheter was introduced over the antegrade wire and inflated in the subintimal space to create a channel between the two different subintimal spaces (arrowheads). (D) After deflation of the balloon catheter (arrowheads), the retrograde guidewire successfully passed through the common channel (arrow). (E) The retrograde guidewire (white arrowheads) entered the true lumen and was captured in the popliteal artery using a 4-Fr catheter (black arrowheads) to establish a through-and-through rail. (F) Post-procedural angiography following balloon angioplasty demonstrates successful revascularization of the anterior tibial artery.
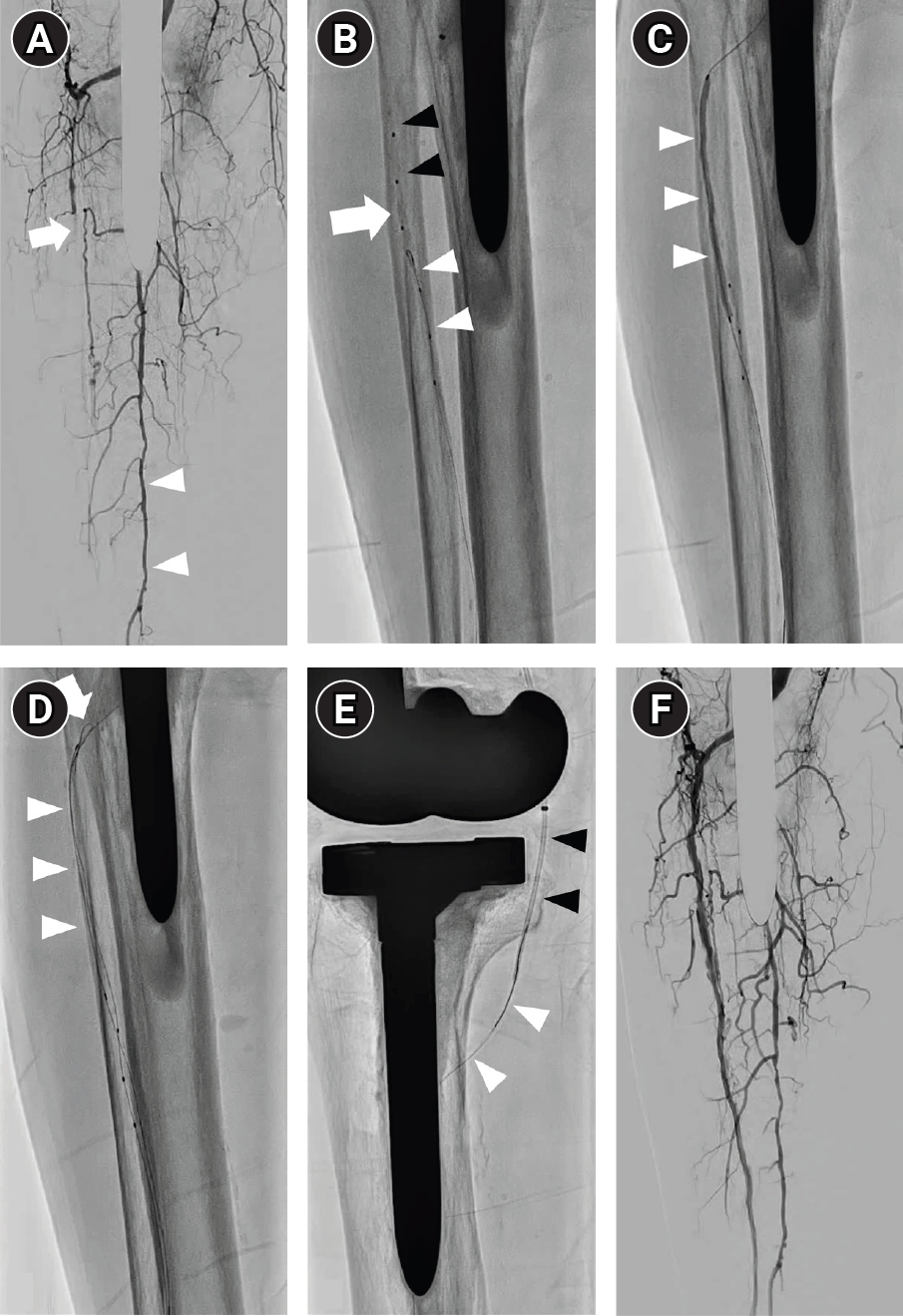
Fig. 2.Pedal arch anatomy. The deep plantar arch (arrowhead) is demonstrated on lateral (A) and anteroposterior (B) pedal angiography. ATA, anterior tibial artery; PTA, posterior tibial artery; DPA, dorsalis pedis artery; LPA, lateral plantar artery; MPA, medial plantar artery.
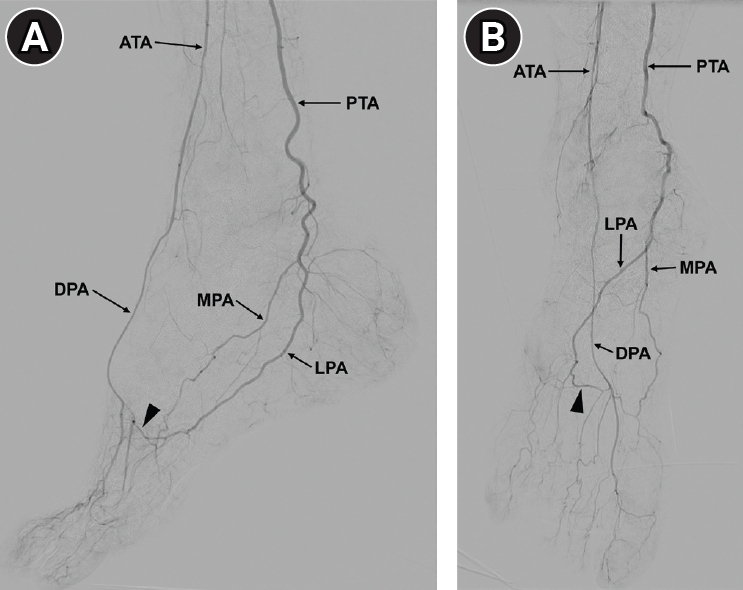
Fig. 3.Procedural workflow for below-the-knee intervention. GW, guidewire; CTO, chronic total occlusion; CART, controlled antegrade and retrograde tracking; PIERCE, percutaneous direct needle puncture of calcified plaque.
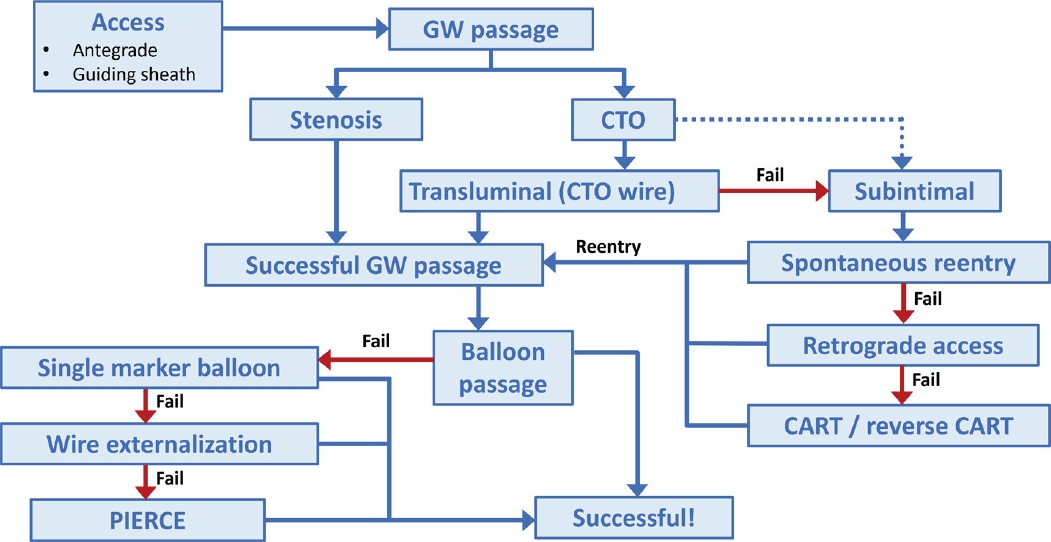
Table 1.Summary of endovascular treatment modalities in BTK disease
Table 1.
|
Modality |
Mechanism |
Key evidence summary |
Clinical considerations |
|
PTA |
Mechanical dilation with a plain balloon |
Remains the reference standard in BTK disease |
Limited by recoil, dissection, and restenosis |
|
DCB |
Mechanical dilation + drug delivery |
Mixed results, without consistent improvement in major clinical outcomes |
Role remains uncertain in BTK disease |
|
DES |
Mechanical support + drug delivery |
Improved patency and reduced TLR in short focal lesions |
Evidence limited in long, diffuse lesions |
|
Bioresorbable scaffolds |
Temporary mechanical support + drug delivery |
Promising early results, but overall evidence remains limited |
Further evidence is required |
|
Atherectomy |
Plaque debulking or modification |
No consistent benefit over PTA in current studies |
Risk of distal embolization; selective use may be considered |
References
- 1. Toledo Barros MG, Fonseca AV, Amorim JE, Vasconcelos V. Retrograde distal access versus femoral access for below the knee angioplasty. Cochrane Database Syst Rev. 2024;1:CD013637. https://doi.org/10.1002/14651858.CD013637.pub2
- 2. Fowkes FG, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382:1329-1340. https://doi.org/10.1016/S0140-6736(13)61249-0
- 3. Gornik HL, Aronow HD, Goodney PP, Arya S, Brewster LP, Byrd L, et al. 2024 ACC/AHA/AACVPR/APMA/ABC/SCAI/SVM/SVN/SVS/SIR/VESS guideline for the management of lower extremity peripheral artery disease: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2024;149:e1313-e1410. https://doi.org/10.1161/CIR.0000000000001251
- 4. Fereydooni A, Gorecka J, Dardik A. Using the epidemiology of critical limb ischemia to estimate the number of patients amenable to endovascular therapy. Vasc Med. 2020;25:78-87. https://doi.org/10.1177/1358863X19878271
- 5. Armstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res. 2020;13:16. https://doi.org/10.1186/s13047-020-00383-2
- 6. Li J, Varcoe R, Manzi M, Kum S, Iida O, Schmidt A, et al. Below-the-knee endovascular revascularization: A position statement. JACC Cardiovasc Interv. 2024;17:589-607. https://doi.org/10.1016/j.jcin.2023.11.040
- 7. Fernandez N, McEnaney R, Marone LK, Rhee RY, Leers S, Makaroun M, et al. Multilevel versus isolated endovascular tibial interventions for critical limb ischemia. J Vasc Surg. 2011;54:722-729. https://doi.org/10.1016/j.jvs.2011.03.232
- 8. Fitridge R, Chuter V, Mills J, Hinchliffe R, Azuma N, Behrendt CA, et al. Editor's choice - The Intersocietal IWGDF, ESVS, SVS guidelines on peripheral artery disease in people with diabetes mellitus and a foot ulcer. Eur J Vasc Endovasc Surg. 2023;66:454-483. https://doi.org/10.1016/j.ejvs.2023.07.020
- 9. Mazzolai L, Teixido-Tura G, Lanzi S, Boc V, Bossone E, Brodmann M, et al. 2024 ESC guidelines for the management of peripheral arterial and aortic diseases. Eur Heart J. 2024;45:3538-3700. https://doi.org/10.1093/eurheartj/ehae179
- 10. Struczewska P, Razian SA, Townsend K, Jadidi M, Shahbad R, Zamani E, et al. Mechanical, structural, and physiologic differences between above and below-knee human arteries. Acta Biomater. 2024;177:278-299. https://doi.org/10.1016/j.actbio.2024.01.040
- 11. Akers NM, Dugas TR. Peripheral artery disease and local drug delivery: a review of disease pathology and drug delivery systems for therapy below the knee. Exp Biol Med (Maywood). 2025;250:10754. https://doi.org/10.3389/ebm.2025.10754
- 12. Kato T, Torii S, Nakamura N, Aihara K, Terabe Y, Iida O, et al. Pathological analysis of medial and intimal calcification in lower extremity artery disease: impact of hemodialysis. JACC Adv. 2023;2:100656. https://doi.org/10.1016/j.jacadv.2023.100656
- 13. Lichtenberg M, Patrone L, Rammos C, Stavroulakis K, Bailey C, Herbert J, et al. Recoil, dissection, and restenosis in Below-The-Knee (BTK) arteries following standard balloon angioplasty. Vasa. 2025 Nov 18 [Epub]. https://doi.org/10.1024/0301-1526/a001254
- 14. Tirziu D, Saleh A, Huang H, Akhlaghi N, Breen TJ, Parikh SA, et al. Safety and efficacy of endovascular treatment modalities for below-the-knee arterial disease: a systematic review and network meta-analysis. J Endovasc Ther. 2025 Jun 30 [Epub]. https://doi.org/10.1177/15266028251344809
- 15. Spiliopoulos S, Del Giudice C, Manzi M, Reppas L, Rodt T, Uberoi R. CIRSE standards of practice on below-the-knee revascularisation. Cardiovasc Intervent Radiol. 2021;44:1309-1322. https://doi.org/10.1007/s00270-021-02891-5
- 16. Tummala S, Briley K. Advanced limb salvage: pedal artery interventions. Semin Vasc Surg. 2022;35:200-209. https://doi.org/10.1053/j.semvascsurg.2022.04.007
- 17. Tan M, Ueshima D, Urasawa K, Hayakawa N, Dannoura Y, Itoh T, et al. Prediction of successful guidewire crossing of below-the-knee chronic total occlusions using a Japanese scoring system. J Vasc Surg. 2021;74:506-513. https://doi.org/10.1016/j.jvs.2021.01.059
- 18. Tan M, Ueshima D, Iida O, Soga Y, Tobita K, Hayakawa N, et al. Clinical validity of the Japanese below-the-knee chronic total occlusion scoring system for the prediction of successful guidewire crossing. J Vasc Surg. 2024;80:1786-1795. https://doi.org/10.1016/j.jvs.2024.07.025
- 19. Ysa A, Lobato M, Patrone L, Arruabarrena A, Monasterio A, Metcalfe M, et al. Tips and tricks for simple and complex below-the-ankle punctures. J Endovasc Ther. 2025;32:1846-1856. https://doi.org/10.1177/15266028241234506
- 20. Troisi N, Turini F, Chisci E, Ercolini L, Frosini P, Lombardi R, et al. Impact of pedal arch patency on tissue loss and time to healing in diabetic patients with foot wounds undergoing infrainguinal endovascular revascularization. Korean J Radiol. 2018;19:47-53. https://doi.org/10.3348/kjr.2018.19.1.47
- 21. Jung HW, Ko YG, Hong SJ, Ahn CM, Kim JS, Kim BK, et al. Editor's choice: impact of endovascular pedal artery revascularisation on wound healing in patients with critical limb ischaemia. Eur J Vasc Endovasc Surg. 2019;58:854-863. https://doi.org/10.1016/j.ejvs.2019.07.034
- 22. Lobato M, Ysa A, Villani F, Chisci E, Michelagnoli S, Patrone L. The guidewire crosses but nothing else does: a pictorial review. Vasa. 2026;55:40-48. https://doi.org/10.1024/0301-1526/a001251
- 23. Delgadillo D, Liang T, Hegazi M, Sharma N, Kabutey NK. In the loop: endovascular pedal arch revascularization. Ann Vasc Surg. 2024;107:84-92. https://doi.org/10.1016/j.avsg.2023.12.099
- 24. McGuirl D, Giles KA. Retrograde tibio-pedal access for endovascular interventions for treating peripheral arterial disease. Ann Vasc Surg. 2024;107:136-139. https://doi.org/10.1016/j.avsg.2023.12.105
- 25. Ichihashi S, Sato T, Iwakoshi S, Itoh H, Kichikawa K. Technique of percutaneous direct needle puncture of calcified plaque in the superficial femoral artery or tibial artery to facilitate balloon catheter passage and balloon dilation of calcified lesions. J Vasc Interv Radiol. 2014;25:784-788. https://doi.org/10.1016/j.jvir.2014.01.016
- 26. Takei T, Miyamoto A, Takagi T, Yamauchi Y. A novel technique of percutaneous intraluminal cracking using a puncture needle for severe calcified lesions of below-the-knee and below-the-ankle arteries. Diagn Interv Radiol. 2021;27:413-417. https://doi.org/10.5152/dir.2021.20675
- 27. Liistro F, Reccia MR, Angioli P, Ducci K, Ventoruzzo G, Falsini G, et al. Drug-eluting balloon for below the knee angioplasty: five-year outcome of the DEBATE-BTK randomized clinical trial. Cardiovasc Intervent Radiol. 2022;45:761-769. https://doi.org/10.1007/s00270-022-03104-3
- 28. Modi K, Joseph T, Shah R, Ranga R, Markel L. Drug-coated balloon angioplasty versus percutaneous transluminal angioplasty for below-the-knee interventions in chronic limb-threatening ischemia patients: systematic review and meta-analysis. Ann Vasc Surg. 2026;123:104-118. https://doi.org/10.1016/j.avsg.2025.09.022
- 29. Cai H, Dong J, Ye Y, Song Q, Lu S. Safety and efficacy of drug-coated balloon in the treatment of below-the-knee artery: a meta-analysis. J Surg Res. 2022;278:303-316. https://doi.org/10.1016/j.jss.2022.04.055
- 30. Fransson T, Mohammed Y, Gottsater A, Resch T. Prospective randomized clinical trial comparing paclitaxel-coated balloon versus conventional balloon angioplasty in treating below the knee arterial lesions in chronic limb threatening ischemia: the CRURAL DEB study. J Endovasc Ther. 2025 Nov 20 [Epub]. https://doi.org/10.1177/15266028251388746
- 31. Zeller T, Baumgartner I, Scheinert D, Brodmann M, Bosiers M, Micari A, et al. Drug-eluting balloon versus standard balloon angioplasty for infrapopliteal arterial revascularization in critical limb ischemia: 12-month results from the IN.PACT DEEP randomized trial. J Am Coll Cardiol. 2014;64:1568-1576. https://doi.org/10.1016/j.jacc.2014.06.1198
- 32. Zeller T, Beschorner U, Pilger E, Bosiers M, Deloose K, Peeters P, et al. Paclitaxel-coated balloon in infrapopliteal arteries: 12-month results from the BIOLUX P-II randomized trial (BIOTRONIK'S-First in Man study of the Passeo-18 LUX drug releasing PTA balloon catheter vs. the uncoated Passeo-18 PTA balloon catheter in subjects requiring revascularization of infrapopliteal arteries). JACC Cardiovasc Interv. 2015;8:1614-1622. https://doi.org/10.1016/j.jcin.2015.07.011
- 33. Patel A, Irani FG, Pua U, Tay KH, Chong TT, Leong S, et al. Randomized controlled trial comparing drug-coated balloon angioplasty versus conventional balloon angioplasty for treating below-the-knee arteries in critical limb ischemia: the SINGA-PACLI trial. Radiology. 2021;300:715-724. https://doi.org/10.1148/radiol.2021204294
- 34. Dadrass F, Raja SC, Lookstein R. Below-the-knee stents and scaffolds: a comprehensive review. Semin Intervent Radiol. 2023;40:167-171. https://doi.org/10.1055/s-0043-57263
- 35. Bosiers M, Scheinert D, Peeters P, Torsello G, Zeller T, Deloose K, et al. Randomized comparison of everolimus-eluting versus bare-metal stents in patients with critical limb ischemia and infrapopliteal arterial occlusive disease. J Vasc Surg. 2012;55:390-398. https://doi.org/10.1016/j.jvs.2011.07.099
- 36. Scheinert D, Katsanos K, Zeller T, Koppensteiner R, Commeau P, Bosiers M, et al. A prospective randomized multicenter comparison of balloon angioplasty and infrapopliteal stenting with the sirolimus-eluting stent in patients with ischemic peripheral arterial disease: 1-year results from the ACHILLES trial. J Am Coll Cardiol. 2012;60:2290-2295. https://doi.org/10.1016/j.jacc.2012.08.989
- 37. Bosiers MJ, Deloose K, Peeters P, Torsello G, Zeller T, Scheinert D, et al. Outcome of a drug-eluting stent in longer below-the-knee lesions in patients with critical limb ischemia. J Cardiovasc Surg (Torino). 2017;58:49-54. https://doi.org/10.23736/S0021-9509.16.09546-X
- 38. Giaquinta A, Vincenzo A, De Marco E, Veroux M, Veroux P. Everolimus-eluting stent for patients with critical limb ischemia and infrapopliteal arterial occlusive disease. Vasc Endovascular Surg. 2017;51:60-66. https://doi.org/10.1177/1538574416689429
- 39. Huizing E, Kum S, Ipema J, Varcoe RL, Shah AP, de Vries JP, et al. Mid-term outcomes of an everolimus-eluting bioresorbable vascular scaffold in patients with below-the-knee arterial disease: a pooled analysis of individual patient data. Vasc Med. 2021;26:195-199. https://doi.org/10.1177/1358863X20977907
- 40. Varcoe RL, DeRubertis BG, Kolluri R, Krishnan P, Metzger DC, Bonaca MP, et al. Drug-eluting resorbable scaffold versus angioplasty for infrapopliteal artery disease. N Engl J Med. 2024;390:9-19. https://doi.org/10.1056/NEJMoa2305637
- 41. DeRubertis BG, Varcoe RL, Krishnan P, Bonaca MP, O'Connor DJ, Pin R, et al. Drug-eluting resorbable scaffold versus balloon angioplasty for below-the-knee peripheral artery disease: 2-year results from the LIFE-BTK trial. Circulation. 2025;152:1076-1086. https://doi.org/10.1161/CIRCULATIONAHA.125.075080
- 42. Benfor B, Sinha K, Lumsden AB, Roy TL. Scoping review of atherectomy and intravascular lithotripsy with or without balloon angioplasty in below-the-knee lesions. J Vasc Surg Cases Innov Tech. 2023;9:101185. https://doi.org/10.1016/j.jvscit.2023.101185
- 43. Zilinyi RS, Alsaloum M, Snyder DJ, Raja A, Mintz AJ, Sethi SS, et al. Surgical and endovascular therapies for below-the-knee peripheral arterial disease: a contemporary review. J Soc Cardiovasc Angiogr Interv. 2024;3:101268. https://doi.org/10.1016/j.jscai.2023.101268
- 44. Feldman ZM, Mohapatra A. Endovascular management of complex tibial lesions. Semin Vasc Surg. 2022;35:190-199. https://doi.org/10.1053/j.semvascsurg.2022.04.008