중심단어
Type II endoleak, transcaval approach, abdominal aortic aneurysm
한글 초록
Type II endoleak 은 복부대동맥류의 인조혈관 스텐트설치술 후에 발생할 수 있는 가장 흔한 합병증이다. 저자들은 복부대동맥류에 대하여 인조혈관 스텐트로 치료받은 뒤 경과 관찰중인 63세 남환에서 발견된 허리동맥을 통한 type II endoleak 에 대하여
transcaval approach 를 이용한 색전술로 치료한 증례를 보고하고자 한다.
영문 초록
Type II endoleak after endovascular repair of an abdominal aortic aneurysm with stent-graft is most common complication. We report a case of a type II endoleak from patent lumbar artery collaterals of the abdominal aortic aneurysm treated with embolization via transcaval approach in a 63-year-old male who was treated with an endovascular stent-graft.
Introduction
복부대동맥류를 인조혈관 스텐트를 이용하여 치료시 대동맥류 내부로의 혈류를 완전히 제거하지 못할 경우 혈관내 누출로 인한 합병증이 생기는 것으로 알려져있다. 그 중에서 측부 혈류를 통한 type II endoleak 은 가장 흔한 합병증으로 대부분 하장간막동맥과 허리동맥을 통한 측부혈류 공급이 원인이 된다. 이러한 type II endoleak 은 대부분 transarterial, transabdominal 혹은translumbar approach 를 이용한 색전술로 치료하게 되지만 앞선 두 방법이 실패한 경우나 적절한 접근 경로가 없을 경우에는transcaval approach 를 통한 색전이 그 대안이 될 수 있다. 우리는 복부대동맥류에 대하여 인조혈관 스텐트를 설치한 환자에서발생한 type II endoleak 에 대하여 transcaval approach 를 이용한 성공적인 치료를 보고하고자 한다.
Case report
증례
63세/남자
임상소견
환자는 신장하 복부대동맥류에 대하여 5개월전 인조혈관 스텐트설치술로 치료받은 뒤 추적 관찰 중 시행한 CT에서 발견된 type II endoleak 의치료를 위하여 의뢰되었음
진단명
Infrarenal abdominal aortic aneurysm, type II endoleak
영상소견
인조혈관 스텐트설치술 후 6개월뒤 시행한 CT에서 복부대동맥에서 양측 총장골동맥까지 인조혈관스텐트가 삽입되어 있었고 스텐트 삽입 전 시행한 CT 와 비교하였을 때 복부대동맥류의 크기가 최대 직경 75mm로 증가하였으며 제3 허리동맥으로부터의 type II endoleak 이 대동맥류 내에서 관찰되고 있었음. (Fig. 1)
시술방법 및 재료
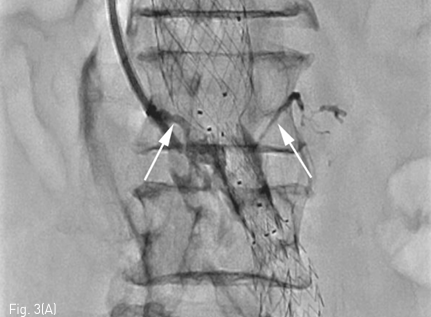
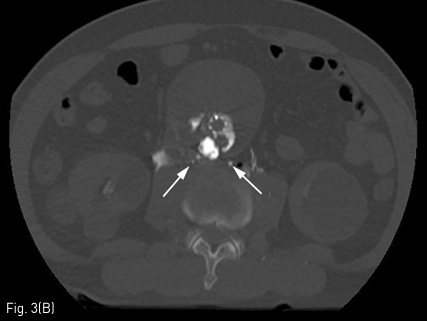
초음파 유도 하에 우측 내경정맥을 천자하여 Rosch-Uchida transjugular liver access set (Cook, Bloomington, IN, USA) 에 포함된 10F sheath 를 하대정맥에 삽입한 뒤 sheath tip 은 제3 요추의 상연에 위치시켰음. 이후 set 에 포함된 14G stiffening cannula에 Rosch-Uchida needle 을 삽입하고 투시의 전후 및 측면 영상을 이용하여 needle의 위치와 천자방향을 확인한 뒤 하대정맥에서 대동맥류를 직접 천자하였음. 이후 needle tip을 동맥류내의 제3-4 요추사이공간 level 의 제3 허리동맥 기시부로 위치시키고 혈관조영술을 시행하였음. 혈관조영술에서 type II endoleak 의 원인이 되는 제3 허리동맥이 관찰되었으며(Fig. 2), 이를 N-butyl cyanoacrylate 와 lipiodol 을 1:2 로 혼합한 용액 4.5mL 를 주입하여 색전술을 시행하였음. 시술 중 시행한 Fluoroscopy 와 시술 후시행한 CT에서 모두 표적인 제3 허리동맥 내부에 lipiodol 이 차 있는 것을 확인한 뒤 시술 종료하였음(Fig. 3)
Fig 1
CT after stent-graft insertion shows type II endoleak and retrograde flow from the right and left lumbar arteries (white arrows)
Fig 2
Angiography after direct puncture of aneurismal sac via transcaval approach revealed contrast filling within the aneurismal sac communicating with lumbar arteries (black arrows)
Fig 3a
Fluoroscopy during the embolization (A) and immediate post-embolization CT (B) shows N-butyl cyanoacrylate and lipiodol mixture fills within the aneurysmal sac and lumbar arteries.
Fig 3b
Fluoroscopy during the embolization (A) and immediate post-embolization CT (B) shows N-butyl cyanoacrylate and lipiodol mixture fills within the aneurysmal sac and lumbar arteries.
고찰
복부대동맥류를 인조혈관 스텐트설치술로 치료시 대동맥류 내부로의 혈류를 완전히 차단하지 못하는 경우에 endoleak 에 의한 합병증이 발생하게 된다. [1] Endoleak 은 그 원인에 따라 4가지 형태로 분류하게 되고 그 중 측부혈류를 통한 type II endoleak 이 가장 흔한 형태로 복부대동맥류로 인조혈관 스텐트설치술을 시행받은 환자의 9%-30%에서 발생한다.[1] 특히 하장간막동맥과 요추동맥이 측부혈류의 원인이 되는 혈관으로서 이를 치료하기 위하여 transarterial, transabdominal, translumbar approach가 주로 사용된다. Baum 등에 따르면 하나의 feeding artery 를 색전할 경우 근처의 다른 혈관으로부터 추가혈류를 공급받아 치료 효과가 낮을 수 있어 다수의 feeding artery 가 있는 경우에는 transabdominal, translumbar approach 와 같이 nidus 역할을 하는 대동맥류를 직접 천자하여 색전하는 방법이 재발률이 더 낮다고 하였다. [2] 최근에 Giancarlo 등은 대동맥류의 크기가 작거나 translumbar approach 시 인조혈관 스텐트를 천자할 수 있는 위험이 큰 경우에 사용할 수있는 transcaval approach 를 소개하였으며 감염의 위험성이 낮다는 것과 누운 상태에서 시술이 이루어지기 때문에 환자가 좀더 편하다는 것을 장점으로 보고하였다.[3, 4] 또한 Ian Jun Yan Wee 등은 transcaval approach를 시행한 증례보고를 취합하여 시술의 안전성과 높은 치료 성공률(80-100%)을 보고하였다.[5-7] 실제로 transcaval approach 시 가능한 합병증으로는 후복막강출혈, 대정맥-대동맥간 누공이 있을 수 있으나 실제로 보고된 바는 없어 그 안전성이 상당히 입증되었다고 생각되며 본 증례에서는 translumbar approach 가 어려운 환자에서 transcaval approach 를 통하여 성공적으로 type II endoleak 을 치료함으로써 그 유용성을 확인하였다.
참고문헌
1. Zener R, Oreop Zener R, Oreopoulos G, Beecroft R, Rajan DK, Jaskolka J, Tan KT. Transabdominal Direct Sac Puncture Embolization of Type II Endoleaks after Endovascular Abdominal Aortic Aneurysm Repair. J Vasc Interv Radiol 2018;29:1167-1173
2. Baum RA, Carpenter JP, Golden MA, et al. Treatment of type 2 endoleaks after endovascular repair of abdominal aortic aneurysms: comparison of transarterial and translumbar techniques. J Vasc Surg 2002;35: 23-29
3. Mansueto G, Cenzi D, D'Onofrio M, Petrella E, Gumbs AA, Mucelli RP. Treatment of type II endoleaks after endovascular repair of abdominal aortic aneurysms: transcaval approach. Cardiovasc Intervent Radiol 2005;28: 641-645
4. Mansueto G, Cenzi D, Scuro A, et al. Treatment of type 4 II endoleak with a transcatheter transcaval approach: results at 1-year follow-up. J Vasc Surg 2007; 45: 1120-1127
5. Scali ST, Vlada A, Chang CK, Beck AW. Transcaval embolization as an alternative technique for the treatment of type II endoleak after endovascular aortic aneurysm repair. J Vasc Surg 2013;57: 869-874
6. Giles KA, Fillinger MF, De Martino RR, Hoel AW, Powell RJ, Walsh DB. Results of transcaval embolization for sac expansion from type II endoleaks after endovascular aneurysm repair. J Vasc Surg 2015;61: 1129-1136
7. Wee IJY, Syn N, Choong AMTL. Transcaval approach for endovascular aortic interventions: A systematic review. J Cardiol 2018;24 doi: 10.1016/j.jjcc. 2018.04.009
Citations
Citations to this article as recorded by