중심단어
Bilioenteric anastomosis creation through percutaneous transjejunal biliary access
국문 초록
간공장문합술과 공장공장문합술을 받았는데, 수술시 오른쪽 담관을 공장과 문합하지 않은 46세 남자 환자이다. 경피경간담즙배액술 및 담도조영술을 하여 이를 확인하였고, 공장을 직접 천자하여 투시 유도하에 오른쪽 담관을 찾아 오른쪽 경피경간담즙배액술 길을 한 개의 유도철사로 연결한 뒤, 돼지꼬리 카테터를 삽입하여 새로운 담관-공장간 길을 만들었다. 이후 점차 굵은 카테터로 바꾸며 길을 넓혔고, 간담도섬광조영술과 담관조영술에서 담즙이 공장으로 잘 빠져나가고 있고 누출이 보이지 않음을 확인하고 카테터를 제거하였다. 재수술을 하지 않고, 공장을 통하여 오른쪽 담관과 공장 사이에 새로운 길을 만든 증례이다.
영문 초록
We report a 46-year-old male patient underwent hepaticojejunostomy and jejunojejunostomy without anastomosing between right hepatic duct and jejunum, which was confirmed by percutaneous transhepatic biliary drainage (PTBD) and cholangiography. Retrograde cannulation of the non-anastomosed right hepatic duct via percutaneous transjejunal access was performed, and the new tract between right IHD and jejunum was secured by a pigtail catheter through right PTBD route via through�and-through technique. Gradual upsizing of the catheter was performed with 8-week intervals. In follow-up hepatobiliary scintigraphy and cholangiography, the bile excretion through the new tract without leak was confirmed, and the catheter was removed. This is a case of a new anastomosis tract creation between the right IHD and the jejunum through percutaneous transjejunal retrograde biliary access, thus preventing reoperation.
Introduction
Percutaneous transjejunal biliary access (PTJBA)는 간공장문합술 등의 수술 후의 담도계 질환 치료를 위한 접근 방법으로, 경피경간 담도배액술 (PTBD) 등의 고식적인 접근이 어려울 때 유용한 접근 방법이다 (1). 우리는 PTJBA를 이용하여, 간공장문합술 시 문합되지 않은 한쪽 담관과 공장 사이의 새로운 길을 만든 1례를 보고한다.
Case report
증례
46세/남자
임상소견
타원에서 급성 쓸개염으로 복강경쓸개절제술을 받던 도중 발생한 총담관 손상으로 전원되었다. 개복하여 간공장문합술과 공장공장문합술을 받은 이후 약 1주일 후에도 담즙이 일 300 cc 이상 배액되어 CT를 촬영하였다.
진단명
Non-anastomosed state of right hepatic duct after hepaticojejunostomy
영상소견
CT (Fig. 1)에서 간공장문합부로 생각되는 부위에 complicated fluid가 보였다. 담즙 우회 (biliary diversion)를 위해 B6 bile duct에 대해 PTBD를 하였다. 시술중 얻은 담관조영술 (Fig. 2)에서는, right IHD만 조영되었고 left IHD는 조영되지 않았다. 또한 공장은 전혀 조영되지 않고 복강으로 조영제가 유출되는 것을 관찰하였다. 한 개의 담관을 공장과 문합하였다는 수술 소견을 참고하여, left IHD만 공장과 문합하고 right IHD는 공장과 문합되어 있지 않음을 알 수 있었다. 환자는 추가적인 수술적 치료를 거부한 상태로, 공장을 직접 천자하는 PTJBA를 통하여 right hepatic duct 접근을 하기로 하였다 (Fig. 3).
시술방법 및 재료
21G 천자침 (Cook, Bloomington, IN, USA)을 이용하여 초음파와 투시 유도하에 공장을 천자하였다. 천자침을 움직이며 조영제를 주입하다가, left hepatic duct를 조영하였다 (Fig. 4A). 그 자리에서 cone beam CT를 촬영하여 (Fig. 4B), 도관되어 있는 left IHD의 끝 부분과, 천자할 right IHD 끝 부분 사이의 위치를 파악하였다. 천자침을 이용하여 right IHD가 있을 것으로 생각되는 뒤쪽 안쪽 (posteromedial)의 공장 벽을 천자하여 복강으로 천자침을 내었다. 그 후, 이미 삽입되어 있는 right PTBD 돼지꼬리 카테터의 끝 부분을 투시 유도하에 천자하여 right IHD를 찾는 데 성공하였다. 이후 over-the-wire 기법으로 0.035 inch 유도철사와 5F 카테터를 삽입하여 through and through 기법으로 기존 PTBD 돼지꼬리 카테터가 삽입되어 있던 경로를 통해 유도철사를 빼내는 데 성공하였다 (Fig. 4C). 이후 PTBD tract을 통해 8.5F 돼지꼬리 카테터 (Cook, Bloomington, IN, USA)를 삽입하였고, 그 끝은 공장에 두었다 (Fig. 4D).
추적관찰
8주 뒤 7mm balloon catheter (Mustang; Boston Scientific, MA, USA)를 이용하여 새로 만든 right IHD-jejunum tract를 확장하였고, 돼지꼬리 카테터를 8주 간격으로 10.2F, 12F, 14F 굵기 순으로 교체하면서 새로 만든 길을 유지하였다. 그 후 8주 뒤에, sidehole이 없는 4F 일자형 카테터로 교체하였다. 다시 8주 뒤에 hepatobiliary scintigraphy를 얻었고 (Fig. 5A), 배설에 지연이 있으나 누출은 보이지 않음을 확인하였다. 1일 뒤, 4F 일자형 카테터를 제거하며 얻은 담관조영술 (Fig. 5B)에서, 누출은 보이지 않고 조영제는 공장으로 잘 빠져나가는 것을 관찰하고 카테터를 완전히 제거하였다
Fig. 1.
Fig. 1. Complicated fluid collection was noted around the hepaticojejunostomy site on the preprocedural CT scan (asterisk).
Fig. 2.
Fig. 2. Nonopacification of jejunum and contrast leakage into peritoneal space were noted on cholangiography during percutaneous transhepatic biliary drainage via B6 bile duct.
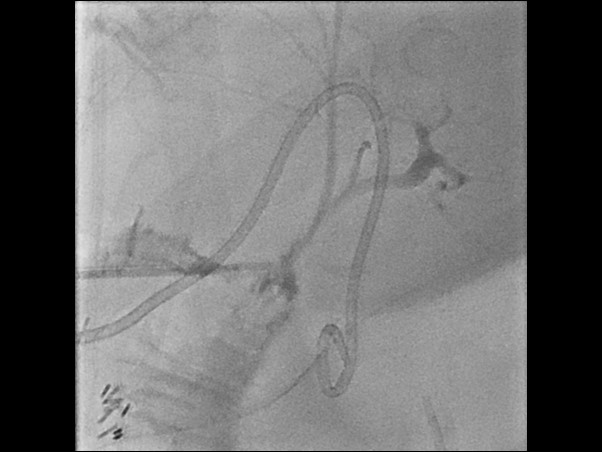
Fig. 3.
Fig. 3. Percutaneous transjejunal biliary access was performed through the curved arrow direction. Right PTBD pigtail catheter and nonanastomosed right IHD was also noted.
Fig. 4. (A)
Fig. 4. (A) Left IHD was cannulated and opacified.
Fig. 4. (B)
(B) Cone beam CT was performed and the anatomic relationship between the cannulated left IHD orifice and right IHD orifice, which was approximated by the neck portion of right PTBD catheter. The right IHD orifice was located on posteromedial direction to the left IHD (arrow).
Fig. 4. C
(C) A guidewire was placed from the transjejunal access site to right PTBD tract with through-and-through technique.
Fig. 4. D
(D) A pigtail catheter was placed through right PTBD tract using the over-the-wire method. The catheter tip was placed in the jejunum (arrow).
Fig. 5. A
Fig. 5.(A) Hepatobiliary scintigraphy showed good hepatic uptake and excretion without leakage.
Fig. 5. B
(B) Cholangiography showed good contrast passage into jejunum without evidence of leakage. The 4F sheath was then removed.
고찰
수술 부위는 염증 및 섬유화 등으로 인하여 재수술시 시야를 확보하기 어렵다. 본 증례와 같이 최초 수술시 (복강경쓸개절제술) 담관 손상이 있어서 담즙이 누출되는 경우에는 복막염을 일으키며 구조물들의 구분이 더욱 불명확해지게 된다. 10년 이상의 경력을 가진 외과의였음에도 불구하고, 수술 시야가 충분히 확보되지 않아 left IHD를 common bile duct로 오인하였고, 결국 right IHD는 문합하지 않은 상태로 수술을 마쳤다. Right IHD를 구분하고 다시 공장과 잇는 재수술을 하기에는 광범위한 수술이 필요할 수 있으며, 시야 확보가 어려워 성공 확률이 낮다. 환자 역시 더 이상의 수술적인 치료를 거부하는 상황이었다. PTJBA를 통한 retrograde biliary access는 PTBD를 통한 antegrade biliary access 만으로 담도계 각종 질환의 치료가 어려운 경우 유용한 대안이 될 수 있다 (1-3). 본 증례에서도, PTBD를 통한 antegrade access만으로는 공장까지 접근할 수 없었으므로, PTJBA를 이용하여 retrograde하게 right IHD를 접근할 수 있었다. Serial biliary tract dilation은 주로 benign biliary stricture의 치료로서 보고된 바 있다 (4, 5). 본 증례에서는 PTJBA를 이용하여, 문합되지 않은 담도를 direct cannulation한 뒤 장기간 카테터를 거치하는 방법으로 담도-공장간 길을 만들었으며, 재수술이 어려운 경우 좋은 대안이 될 수 있다.
참고문헌
1. Kim D, Bolus C, Iqbal SI, Davison BD, Ahari HK, Flacke S, et al. Percutaneous Transjejunal Biliary Access in 60 Patients with Bilioenteric Anastomoses. J Vasc Interv Radiol 2019;30:76-81.e71
2. Fontein DB, Gibson RN, Collier NA, Tse GT, Wang LL, Speer TG, et al. Two decades of percutaneous transjejunal biliary intervention for benign biliary disease: a review of the intervention nature and complications. Insights Imaging 2011;2:557-565
3. Lopera JE, Ramsey GR. Transjejunal biliary interventions: going back to a road less traveled. Acta Radiol 2014;55:1210-1218
4. Gwon DI, Sung KB, Ko GY, Yoon HK, Lee SG. Dual catheter placement technique for treatment of biliary anastomotic strictures after liver transplantation. Liver Transpl 2011;17:159-166
5. Reis SP, Bruestle K, Brejt S, Tulin-Silver S, Frenkel J, Mobley DG, et al. Evaluation of a three-session biliary dilation protocol following transplant-related biliary stricture in pediatric patients. Pediatr Transplant 2019;23:e13551
Citations
Citations to this article as recorded by