중심단어
Atherosclerosis obliterance, common iliac artery, subintimal recanalization, Outback reentry catheter
임상소견
내원 5년전부터 지속된 좌측하지의 파행으로 내원함. 과거력상 당뇨, 고혈압, 안정성 협심증 있으며 ABI는 0.76(우측)八).49(좌측)으로 측정됨.
진단명
양측 총장골동맥과 좌측 외장골동맥의 동맥경화 폐쇄증
영상소견
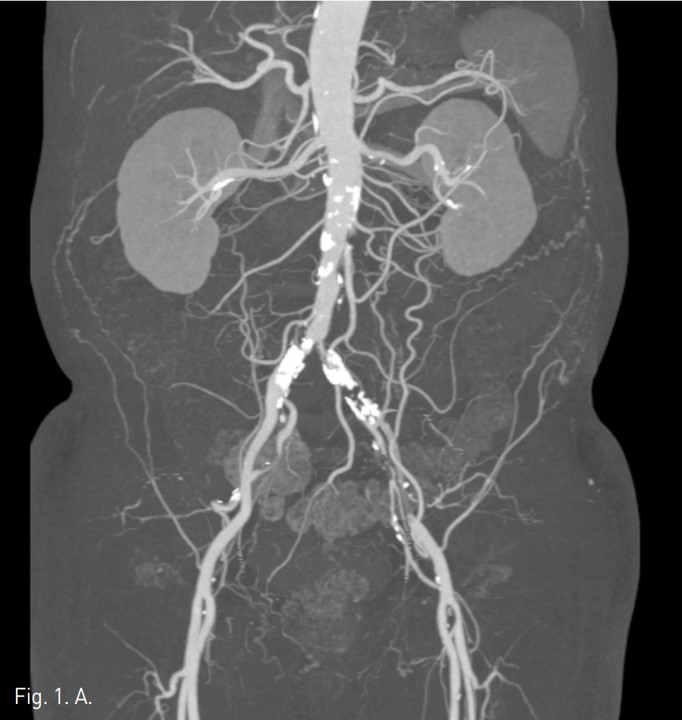
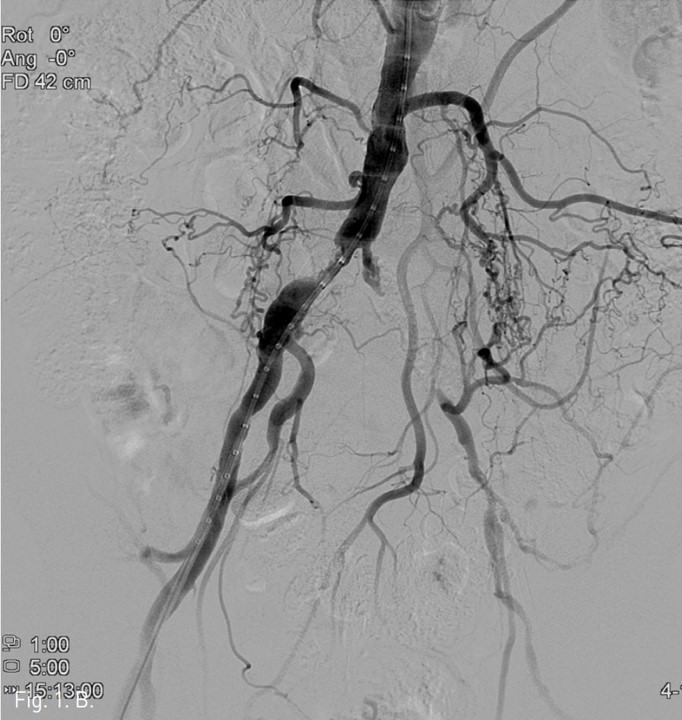
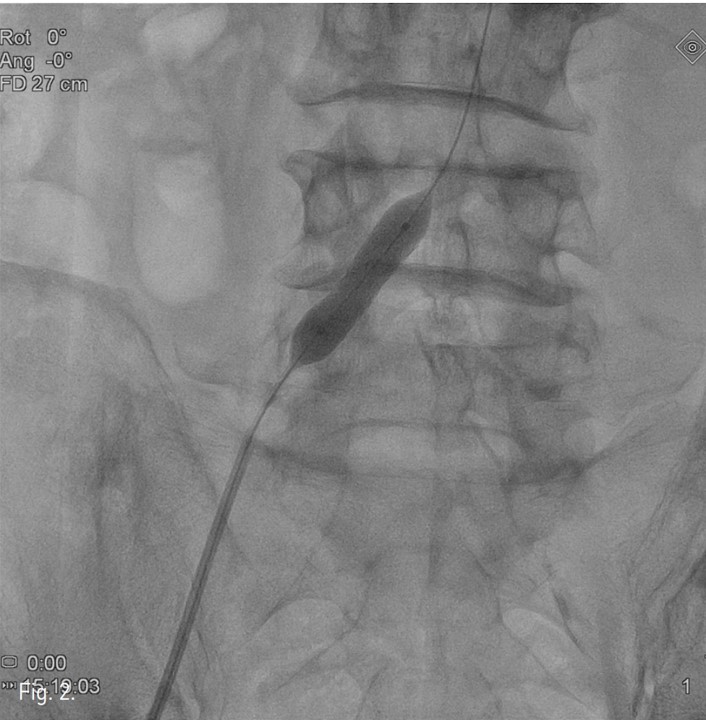
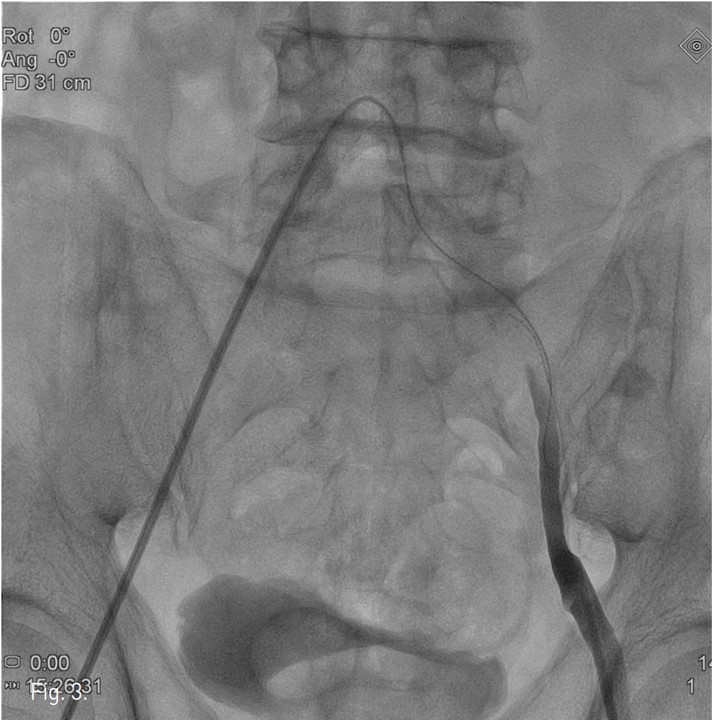
컴퓨터단층촬영 혈관조 영술과 고식적 혈관조영술에서 우측 총장골동맥에 석회화를 동반한 80%정도의 심한 협착이 있고, 좌측 총장골동맥에서 외장골동맥에 석회화를 동반한 완전 폐쇄의 소견이 있다 (Fig. 1A, IB). 우총대퇴동맥의 근위부에 10mm x 29mm Zenesis stent를 설치하였다 (Fig. 2). 0.035 inch guidewire로 좌측 총장골동맥의 기시부 폐쇄부위 통과를 시도하였으나 가성내강에서 진성내강으로 재진입이 되지 않았다 (Fig. 3). 좌측 외장골동맥 진성내강 내에 있는 ‘L-자’ 표시방향의 outback device가 보인다 (Fig. 4A), 좌측 외장골동맥 진성내강 내에 있는 'T-자’ 표시방향의 outback device가 보인다(Fig. 4B). Outback device를 이용하여 동맥내막을 천자후 0.014 inch guidewire를 가성내강 내로 진입시켰지만 좌측 총장골동맥-외장골동맥경 계부위에서 더 이상 진행되지 않았다 (Fig. 4C). 0.014 inch guidewire를 따라서 Davis catheter를 가성내강 내로 진입시키고 (Fig. 5A), 10mm snare를 삽입하여 Simmon catheter내부에 있던 microwire를 전진시켜 snare로 잡아 좌측 sheath로 뽑아내어 (Fig. 5B), 5Fr. Davis catheter를 대동맥 내부로 진입시켰다(Fig. 5C). 양측 총장골동맥 및 좌측 외장골동맥 스텐트 설치후 대동맥장골동맥조영술상에서 양측 장골동맥의 완전한 재개통을 보인다 (Fig. 6).
시술방법 및 재료
초음파 유도하에 양측 총대퇴동맥을 역방향 천자하고 7Fr. arterial sheath를 삽입한후 pigtail catheter (Cordis, Miami Lakes, FL, USA)를 이용하여 대동맥장골동맥조영술을 시행하여 우측 근위부 총장골동맥의 80%정도의 협착과 좌측 근위부 총장골동맥의 완전폐쇄를 확인하였다. 이어 우총대퇴 동맥의 심한 협착에 대하여 10 mm x 29 mm (deploy시 25 mm) Zenesis stent (Cordis)를 설치하였다.
우측 arterial sheath를 통하여 좌측 총장골동맥의 기시부에 Simmon catheter(A&A M.D., Seongnam-si, Korea)를 위치시키고 0.035 inch guide wire (Terumo, Tokyo, Japan) 로 폐쇄부위 통과를 시도하였으나 가성내강에서 진성내강으로 재진입이 되지 않았다.
Outback device사용을 위해, 우측 arterial sheath를 통하여 위치하고 있는 Simmon catheter 내부의 0.035 inch guidewire를 제거하고 microcatheter (Cook, Bjaeverskov, Denmark)를 위치시킨 후, 조영제를 주입하여 가성내강의 위치를 확인하고, 좌측 arterial sheath로 조영제를 주입하여 좌측 외장골동맥의 진성내강의 위치를 확인하였다.
좌즉 arterial sheath내부로 outback device를 전진하여 ‘L-자’ 표시를 확인하고, tube를 90도 회전하여 'T-자’ 표시를 확인한 후, outback device의 바늘로 천자 후 0.014 inch Trenscend guide wire(Boston scientific, Miami, USA)를 가성내강 내로 진입시켰지만 좌측 총장골동맥과 외장골동맥의 경계부위 부터 대동맥으로 진입되지 않았다.
0.014 inch guidewire를 따라서 5Fr. Davis catheter(A&A M.D.)를 가성내강내로 진입시키고 10mm snare를 삽입한 후 Simmon catheter 내부에 있던 microwire를 후진하였다가 전진하여 snare로 잡아 좌측 sheath로 뽑아내어 through-and-through technique으로 Davis catheter를 대동맥 내부로 진입시킬 수 있었다.
좌측 총장골동맥 및 외장골동맥에 대하여 6mm x 4cm power flex P3 balloon(Cordis)으로 preballooning을 시행한 후 10mm x 6cm Smart control stent(Cordis)를 근위부부터 총장골동맥에 삽입하고 10mm x 8cm Zilver stent (Cook)를 외장골동맥에 삽입하였다. 이후 좌측 총장골동맥에는 9mm x 4cm Powerflex P3 balloon (Cordis) 으로, 외장골동맥에는 7mm x 4cm Powerflex P3 balloon(Cordis)으로 stent내부에서 풍선확장술을 시행하였다.
시술 후 대동맥장골동맥조영술상에서 양측 장골동맥의 완전한 재개통을 보인다.
고찰
총장골동맥의 완전폐색인 경우 역방향으로 outback device를 내막하 가성내강으로 진입시켜 대동맥분기의 직상방에서 대동맥강 내의 진성내강으로 천자하는것이 일반적인 방법이다.
본 증례에서는 총장골동맥의 stump가 있어서 순방향으로 0.035 inch guidewire를 사용하여 내막하경로로 진행하였으나 재진입이 되지 않았다. 또한 대동맥장골동맥 분지부위가 예각을 이루고 있어 우측 arterial sheath로 outback device를 넣어서 좌측 외장골동맥의 가성내강까지 접근할 수 없다고 판단되어서, 좌즉 arterial sheath로 outback device를 넣어서 진성내강에서 가성내강으로 천자하였으나 가성내강의 길이가 길었으며 불규칙한 공간이므로 0.014 inch guidewire가 대동맥의 진성내강으로 쉽게 나오지 못하였다. 이러한 경우 snare를 사용하여 through-and-through technique으로 해결할 수 있다.
참고문헌
1. Ramjas G, Thuriey P, Habib S. The use of a reentry catheter in recanalizatbn of chronic inflow occlusions of the common iliac artery. Cardio vasc Intervent Radiol. 2008 May-Jun;31(3):650-4.
2. Bozlar U, Shih MC, Harthun NL, Hagspiel KD. Outback catheter-assisted simultaneous antegrade and retrograde access for subritimal recanalization of peripheral arterial occlusion. Clin Imaging. 2008; 32:236-40.
3. Wagner JK, Chaer RA, Rhee RY, Marone LK. True lumen re-entry after extravascular recanalization of a superficial femoral artery chronic total occlusion. J Vasc Surg. 2010; 52:216-8.
4. Etezadi V, Benenati JF, Patel PJ, Patel RS, Powell A, Katzen BT. The reentry catheter: a second chance for endoluminal reentry at difficult bwer extremity subintimal arterial recanalizations J Vasc Interv Radiol. 2010; 21:730-4.
5. Beschorner U, Sixt S, Schwarzwalder U, et al. Recanalization of chronic occlusions of the superficial femoral artery using the Outback reentry catheter a single centre experience. Catheter Cardiovasc Interv. 2009; 74:934-8.
6. Husmann M, Federer J, Keo HH, et al. Bailout revascularization of chronic femoral artery occlusions with the new outback catheter following failed conventional endovascular intervention. J Endovasc Ther. 2009; 16:206-12.
Fig. 1. A
Fig. 1. Enhanced coronal CT angiography MIP image and conventional aortoiliac angiography show about 80% occlusion at right common iliac artery and complete occlusion at left common iliac artery and external iliac artery.
Fig. 1. B
Fig. 1. Enhanced coronal CT angiography MIP image and conventional aortoiliac angiography show about 80% occlusion at right common iliac artery and complete occlusion at left common iliac artery and external iliac artery.
Fig. 2.
Fig. 2. Balloon expandable stent (10mm x 29mm) was deployed at right common iliac artery.
Fig. 3.
Fig. 3. Antegrade subintimal passage of 0.035 inch guidewire into the distal true lumen was failed.
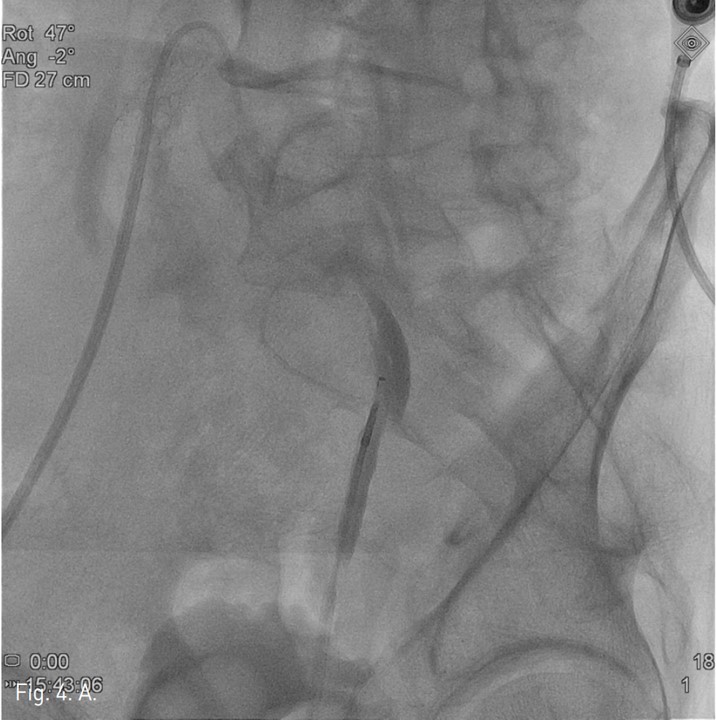
Fig. 4. A
Fig. 4. A. Radiograph taken while L-shaped marker of Outback device is seen.
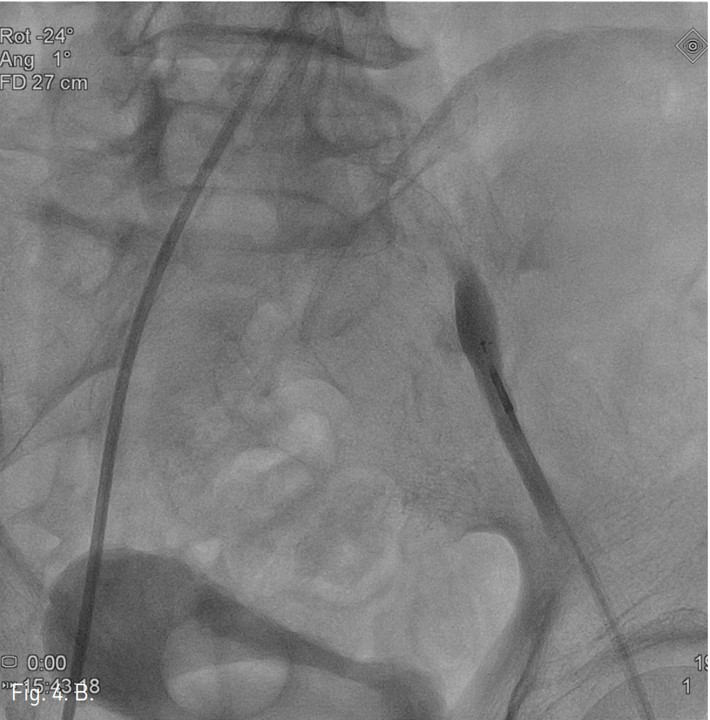
Fig. 4. B
B. Radiography taken while T-shaped marker of Outback device is seen.
Fig. 4. C
C. After intimal puncture using Outback device, a 0.014 inch guidewire was advanced into the false lumen.
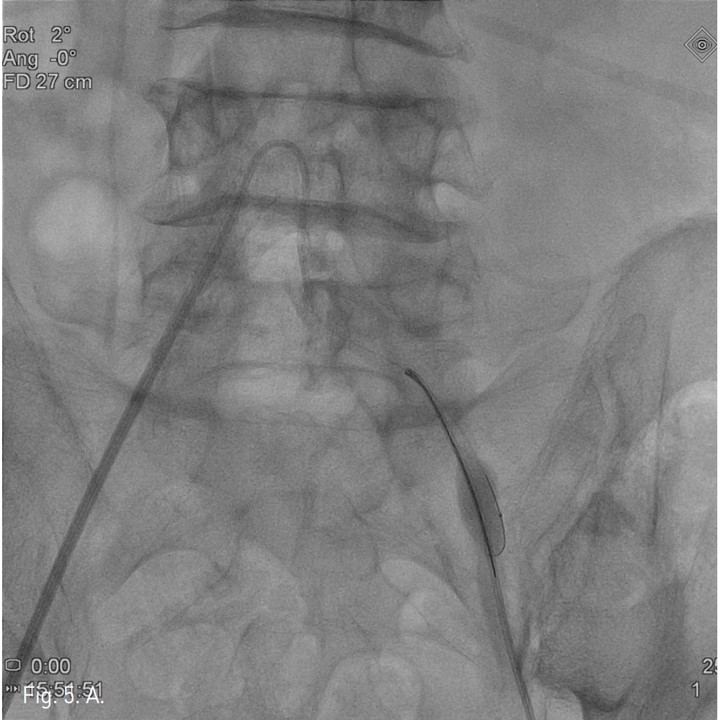
Fig. 5. A
Fig. 5. A and 5B. Radiograph obtained at the moment of capturing proximal microwire using a snare.
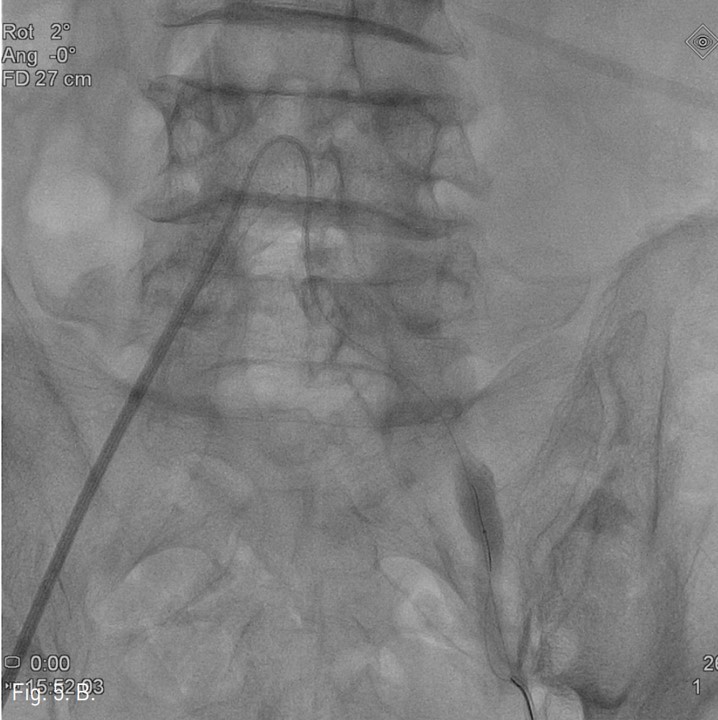
Fig. 5. B
Fig. 5. A and 5B. Radiograph obtained at the moment of capturing proximal microwire using a snare.
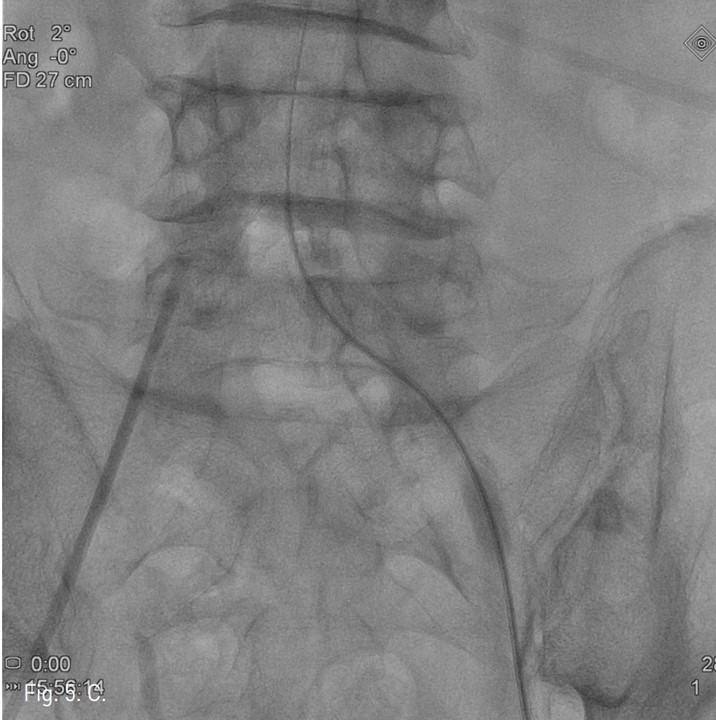
Fig. 5. C
C. Davis catheter was successfully advanced into the aortic true lumen.
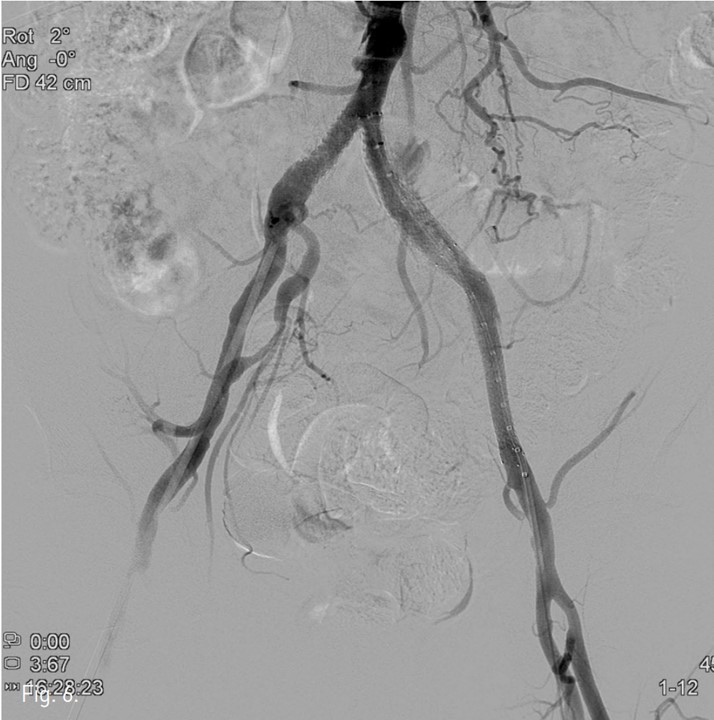
Fig. 6.
Fig. 6. Completion pelvic arteriography shows complete recanalization of both common iliac and left external iliac arteries.
Citations
Citations to this article as recorded by