중심단어
Duodenocaval fistula, inferior vena cava, foreign body.
임상소견
내원 2주 전부터 지속된 발열 및 복통을 주소로 내원함. 복부 컴퓨터단층촬영(CT)에서 12번 흉추골 높이의 하대정맥 내부에 공기방울을 포함한 혈전이 발견됨(크기: 가로 1.4cm, 세로 1.0cm 높이 2.5cm). 위십이지장 내시경상 특이 소견 없었으며, 심부정맥혈전증이나 심혈관계 질환의 증거도 없었음.
진단명
Infected thrombus in IVC (하대정맥 내부의 감염성 혈전증)
영상소견
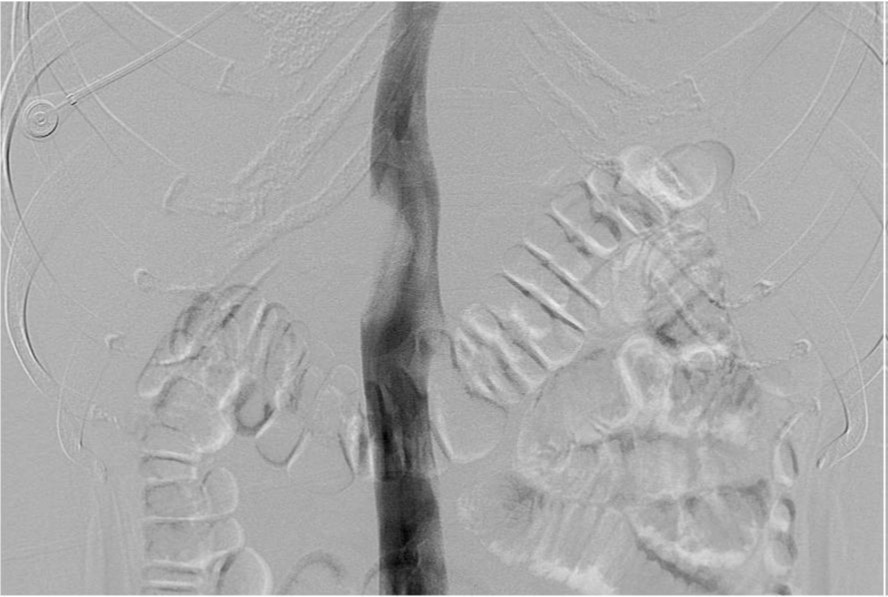
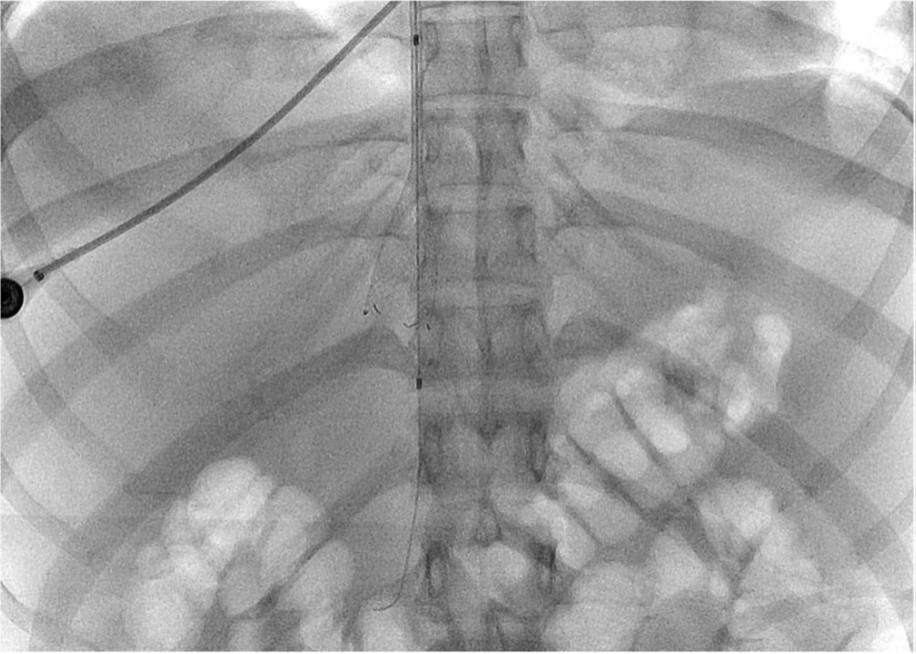
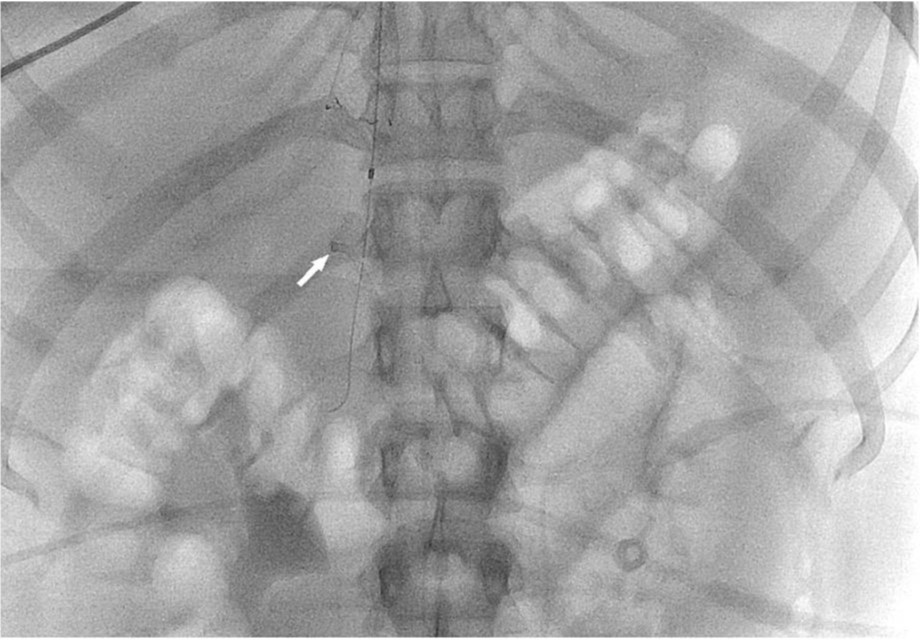
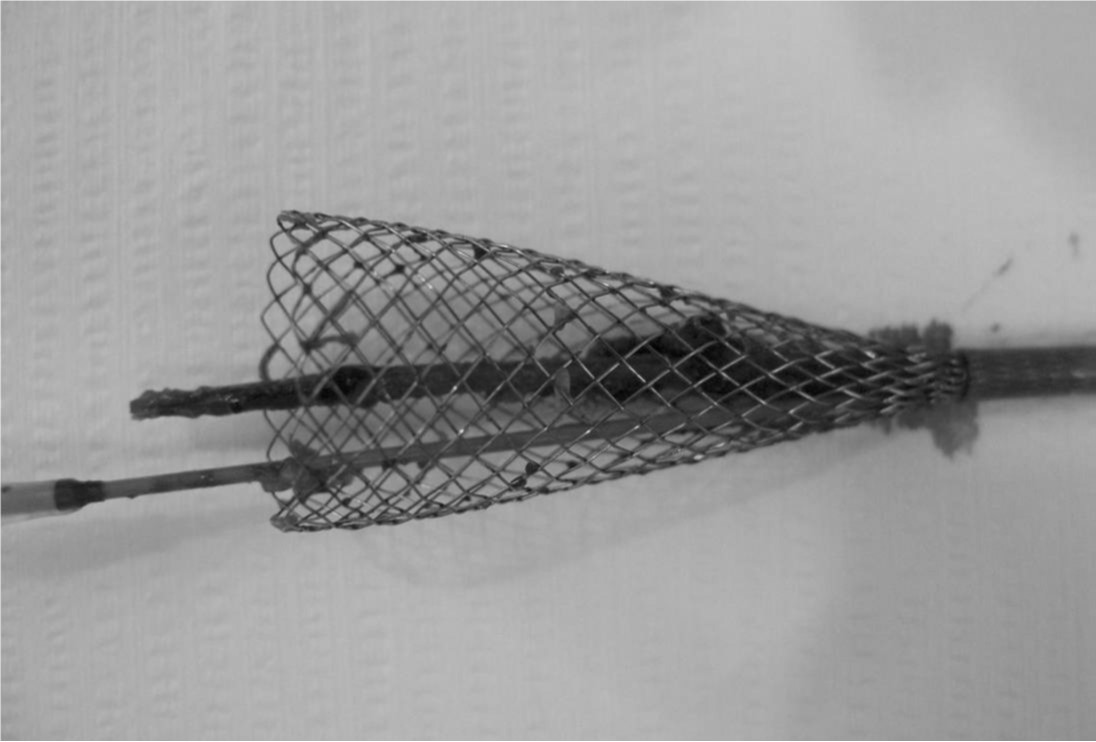
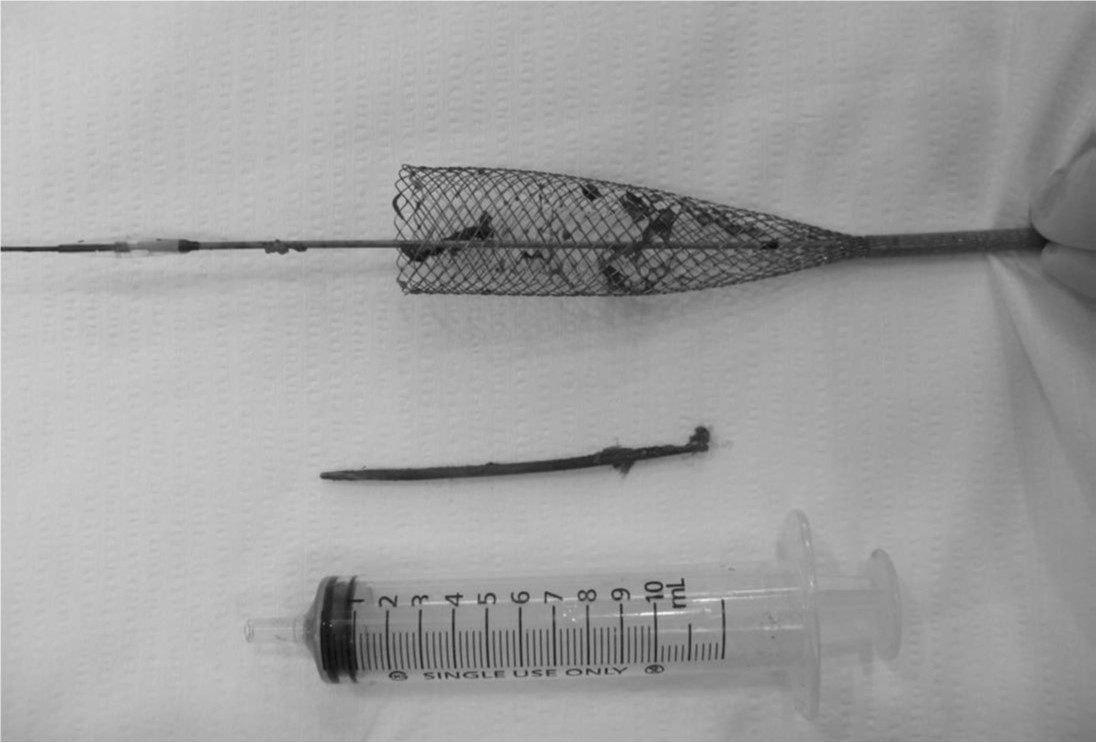
복부 컴퓨터단층촬영에서 12번 흉추골 높이의 하대 정맥에 2.5cm 크기의 공기방울을 포함한 혈전이 있다(Fig. 1A, IB). 하대정맥조영술에서 내경의 50%정도를 채우고 있는 혈전으로 인한 filling defect가 있다 (Fig. 2A). 혈전의 상부에 임시 하대정맥 필터로 Niti-S 스텐트를 삽입한 후 부분적으로(50%) 펼쳤다(Fig. 2B). Renal guiding catheter를 삽입하여 혈전에 대해 수차례 흡인 혈전제거술을 시행하여 다량의 백색혈전을 흡인하였다(Fig. 2C). 이후 시행한 하대정맥조영술에서 혈전의 일부가 스텐트 내부로 이동한 것을 확인하고 스텐트를 재포획하여 혈전을 제거하였다 (Fig. 2D). 스텐트에 혈전 및 나무재질의 이쑤시개가 배출되었다 (Fig. 3A, 3B).
시술방법 및 재료
초음파 유도하에 우총대퇴정맥을 천자하고 12Fr. sheath(ST. Jude. Medical, Minnetonka, USA)를 우총대퇴 정맥에 삽입하고 하대정맥조영술을 시행하여 혈전의 위치를 확인하였다. 초음파 유도하에 우내경정맥을 천자하고 12Fr. sheath(ST. Jude. Medical)를 우내경정맥에 삽입하고 혈전의 상부에 임시 하대정맥 필터로 20mm 직경의 Niti-S vascular stent(Taewoong medical, Gimpo-si, Korea)를 삽입한 후 부분적으로(50%) 펼쳤다. 우총대퇴정맥을 통하여 7Fr Renal double curve guide catheter(Cordis, Miami Lakes, FL, USA)를 혈전에 위치시키고 50cc 주사기로 음압을 가하면서 catheter를 위아래로 움직이며 흡인혈전제거술을 시행하여 다량의 백색혈전을제거하였다. 이후 다시 하대정맥 조영술을 시행하였을 때 흡인되지 않고 남은 혈전이 대부분 스텐트 내부로 이동하였고 스텐트를 재포획하여 혈전을 제거하였다. 외부로 꺼내어진 스텐트 내부에는 약 5cm가량의 나무재질의 이쑤시개가 발견되었다.
고찰
십이지장대정맥루는 드물지만 치명적 인 합병증으로 약 40%의 치명률을 가지는 것으로 보고되고 있으며, 원인으로는 하대정맥 필터의 이동에 따른 합병증, 소화성궤양질환, 방사선 치료, 섭취된 이물질에 의한 것 등이 있다.
증상은 대부분 토혈, 혈변 등 위장관출혈증상이나 폐혈증으로 나타나며, 진단은 내시경에서 십이지장루를 통한 출혈이 보이거나, 컴퓨터단층촬영상 하대정맥 내부의 공기방울을 포함한 혈전, 십이지장과 하대정맥 주위의 감염성 액체저류나 농양, 이물질의 발견이나, 하대정맥 필터의 이동 등이 보일 때 증상과의 연관성에 따라 진단할 수 있다. 그러나 실제로는 십이지장대정맥루의 약 50%의 환자만이 컴퓨터단층촬영으로 진단된다고 한다.
본 환자의 경우도 십이지장대정맥루는 내원 시점에서는 이미 치유되어 내시경이나 CT상 관련 소견은 보이지 않았고, 단지 하대정맥 내부의 공기방울을 포함한 혈전소견 만이 관찰되었다. 또한 흡인 혈전제거술을 시행하여 혈전 및 이물질을 제거하기 전에는 이쑤시개나 십이지장대정맥루의 존재를 알지 못하였고, 단순히 감염성 혈전증만을 의심하였다. 이와 같이 십이지장대정맥루는 치료가 시작되기 전에 미리 진단이 어려운 문제점이 있다.
참고문헌
1. Perera GB, Wilson SE, Barie PS, Butler JA. Duodenocaval fistula: a late complication of retroperitoneal irradiation and vena cava replacement. Ann Vase Surg. 2004;18:52-58.
2. Guillem PG, Binot D, Dupuy—Cuny J, Laberenne JE, Lesage J, Triboulet JP, Chambon JP. Duodenocaval fistula: a life-threatening condition of various origins. J Vase Surg. 2001; 33:643-645.
3. Allen Krupski WC, Wylie EJ. Toothpick perforation of the inferior vena cava. West J Med. 1983; 138:727-730.
4. Benjamin DS, Ruckle HC, Hadley HR. Local recurrence of renal cell carcinoma causing duodenal inferior vena caval fistula: case report and review of the literature. Urology. 1996 ;48:636 -638.
5. Rioux M, Lacourciere L, Langis P, Rouleau M. Sonographic detection of ingested foreign bodies in the inferior vena cava. Abdom Imaging. 1997; 22:108-110.
6. Kaufman LB, Yeh BM, Breiman RS, Joe BN, Qayyum A, Coakley BV. Inferior vena cava filling defects on CT and MRI. AJR Am J Roentgenol. 2005; 185:717-726.
7. Godwin TA, Mercer G, Holodny Al. Fatal embolization of intestinal contents through a duodenocaval fistula. Arch Pathol Lab Med. 1991; 115:93-95.
Fig. 1. A
Fig. 1. Enhanced axial and coronal CT scan shows thrombus with air-bubbles in IVC adjacent to duodenal second portion.
Fig. 1. B
Fig. 1. Enhanced axial and coronal CT scan shows thrombus with air-bubbles in IVC adjacent to duodenal second portion.
Fig. 2. A
Fig. 2. A. IVC venogram shows large filling defect due to thrombus.
Fig. 2. B
B. Radiography obtained during partial deployment of stent as a temporary IVC filter.
Fig. 2. C
C. Radiography obtained during aspiration thrombectomy of IVC thrombus by renal guiding catheter.
Fig. 2. D
D. IVC venogram after aspiration thrombectomy shows migrated thrombus entrapped in the partially deployed stent.
Fig. 3. A
Fig. 3. A. A wooden toothpick is captured in the partially deployed stent.
Fig. 3. B
B. A photograph for the retrieved wooden toothpick with 10cc syringe.
Citations
Citations to this article as recorded by