중심단어
Superior mesenteric artery, dissection, stent
임상소견
상복부 통증을 주소로 내원하여 통증의 원인을 찾기 위해 상부 위장관 내시경을 시행하였으나 특이 소견 없어 CT를 시행하였음.
진단명
Spontaneous isolated SMA dissection
영상소견
2009년 3월 복부 CT에서 SMA 기시부 하방 2cm 부위부터 5cm 길이의 편심성 혈전이 관찰되고 있으며 혈전이 있는 부위의 동맥 직경이 커져 있음(Fig. 1). 대동맥이나 분지 동맥에 동맥경화증의 소견은 관찰되지 않으며 심장초음파 및 심전도 검사에서 혈전이나 심방 세동은 없었음. CT 소견과 증상을 기준으로 spontaneous isolated SMA dissection으로 진단하였으며 창자의 허혈 소견이 보이지 않고 통증도 악화되지 않아 보존적 치료를 하였음. 2009년 6월 추적 CT에서 false lumen내 대부분의 혈전은 소실되었으나 SMA 기시부 5cm 하방 부위에는 국소적 혈전을 동반한 saccular pseudoaneurysm이 관찰됨. 2009년 8월 시행한 추적 CT에서 pseudoaneurysm의 직경이 2mm 증가함 (Fig. 2). 2009년 9월 시행한 혈관 조영술에서 saccular pseudoaneurysm이 SMA 기시부 5cm 하방부위에 관찰되며 SMA의 국소적 협착이 관찰됨 (Fig. 3). 스텐트와 코일을 이용한 혈관 내 치료 후 시행한 혈관 조영술에서 SMA의 국소적 협착과 pseudoaneurysm은 소실됨 (Fig. 4). 시술 3개 월 후 시행한 추적 CT에서 pseudoaneurysm은 완전히 소실되었으며 SMA는 정상소견을 보임(Fig. 5).
시술방법 및 재료
Right femoral artery를 천자하여 superior mesenteric artery에 7-Fr guiding catheter(Cordis, FL, USA)를 위치시킨 후 시행한 혈관 조영술에서 SMA dissection 부위 true lumen의 협착과 동반된 pseudoaneurysm이 관찰됨, 협착된 SMA의 true lumen내에 6mm 직경, 29mm 길이의 balloon expandible stent(Genesis, Cordis, FL, USA)를 설치함.
스텐트 설치 후 협착은 소실되었으나 pseudoaneurysm은 소실되지 않고 크기만 작아짐. 스텐트의 철망을 통해 2.4 Fr microcatheter(Progreat, Terumo, Tokyo, Japan)를 pseudoaneurysm내에 위치시킨 다음 5mm microcoil (Cook, Bloomington, IN) 1개를 삽입함. 시술 후 시행한 혈관 조영술에서 SMA 협착과 pseudoaneurysm은 완전히 소실되었으며 추적 관찰기간 동안 재발 소견은 보이지 않음.
고찰
SMA dissection은 carotid artery dissection 다음으로 흔한 말초동맥 박리로 정확한 원인은 잘 알려져 있지 않지만 SMA 기시부에서 1.5-3cm 하방 부위에서 dissection이 시작되는 것으로 보아 비정상적인 shear stress에 의한 혈관 내막 손상과 관련이 있는 것으로 여겨진다. 조영증강 CT에서 intimal flap을 관찰하면 확진을 할 수 있으나 intimal flap을 보이지 않고 mural thrombus만 보이는 경우는 SMA thromboembolism과의 감별이 필요하다. 치료 방법으로는 보존적 치료, 스텐트 설치술, 수술 등이 있으며 최근 Yun 등은 SMA dissection과 연관된 복통의 대부분은 창자의 허혈성 통증이 아닌 dissection에 의한 visceral nerve plexus의 자극으로 발생하므로 보존적 치료만으로도 증상이 호전되며 SMA dissection도 악화되지 않는다고 보고하고 있다. 그러나 본 증례와 같이 false lumen pseudoaneurysm의 직경이 증가하여 SMA rupture의 가능성이 있거나 true lumen의 혈전형성에 의한 acute bowel ischemia가 발생하면 혈관내 스텐트 설치술이나 수술적 치료가 필요하다.
참고문헌
1. Kim JH, Roh BS, Lee YH, et al. Isolated spontaneous dissection of the superior mesenteric artery: percutaneous stent placement in two patients. Korean J Radiol 2004; 5:134-138.
2. Yun WS, Kim YW, Park KB, et al. Clinical and angiographic follow -up of spontaneous isolated superior mesenteric artery dissection. Eur J Vasc Endovasc Surg 2009;37:572-577.
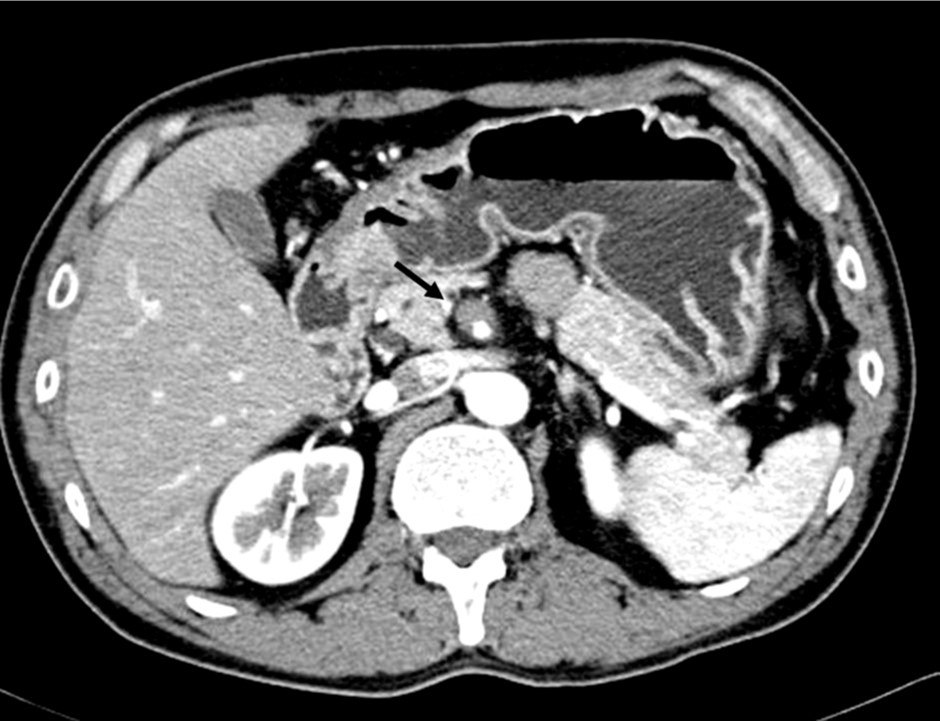
Fig. 1.
Fig. 1. Enhanced CT scan shows eccentric thrombosis in the superior mesenteric artery at the levrd of transition zone from a fixed segment under the pancreas to the mobile segment at the mesenteric root.
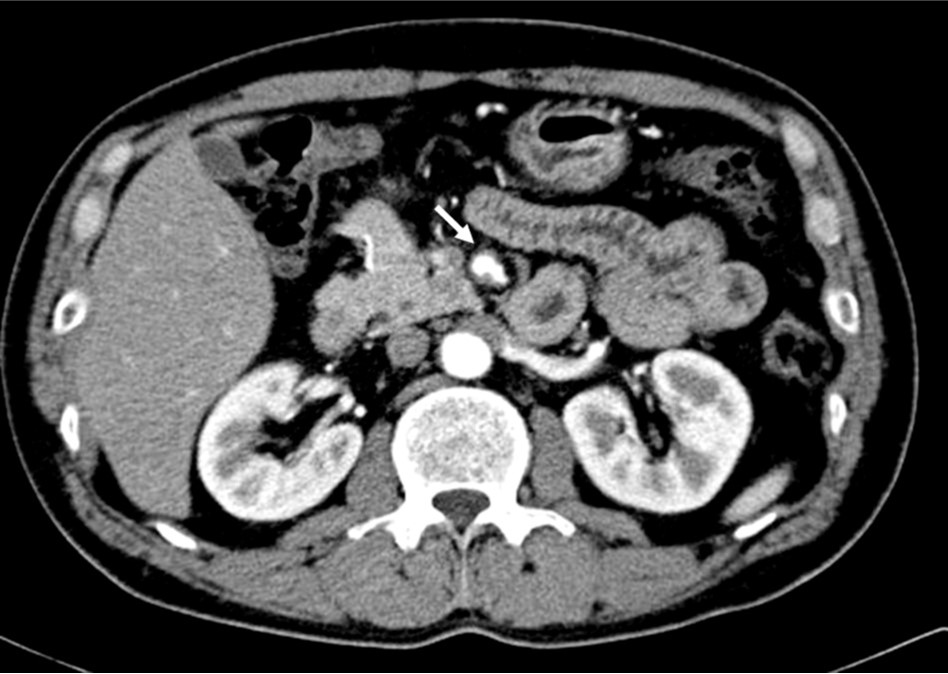
Fig. 2.
Fig. 2. Enhanced CT scan obtained 6 month later reveals improvement of eccentric thrombus, but a saccular pseudoaneurysm is noted in the superior mesenteric artery.
Fig. 3.
Fig. 3. Superior mesenteric angiography shows a saccular pseudoaneurysm with focal stenosis in the superior meseteric artery.
Fig. 4. A
Fig. 4. A. The size of psedoaneurysm is decreased, but still noted after stent placement in the superior mesenteric artery.
Fig. 4. B
B. After insertion of microcatheter in the sac of pseudoaneurysm through the mesh of stent, a 5mm diameter microcoil is placed in the sac.
Fig. 4. C
C. Completion angiography shows improvement of pseudoaneurysm and stenosis in the superior mesenteric artery.
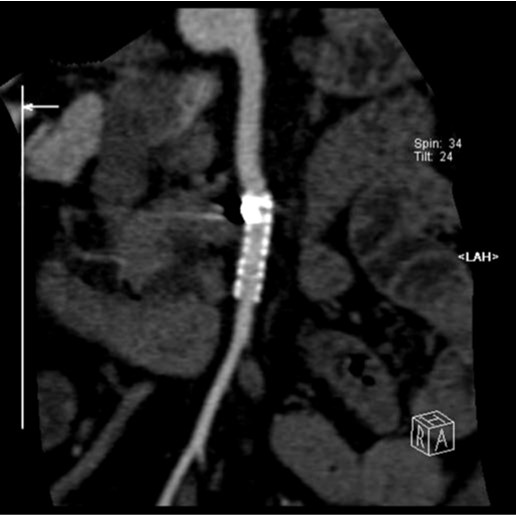
Fig. 5.
Fig. 5. Curved MPR image obtained 3 months after procedure shows complete obliteration of pseudoaneurysm and patent superior mesenteric artery.
Citations
Citations to this article as recorded by