중심단어
Dorsal pancreatic artery, superior mesenteric vein, fistula, pseudoa neurysm, pancreatitis
임상소견
Chronic heavy alcoholics환자로 2주전부터 급성췌장염으로 치료받던 중 갑자기 발생한 복통을 주소로 내원함. 내원 후 시행한 CT상에서 10cm 크기의 혈종과 거짓동맥류(pseudoa neurysm)가 발견되었음.
진단명
Pseudoaneurysm of dorsal pancreatic artery and arteriovenous fistula between dorsal pancreatic artery and superior mesenteric vein
영상소견
내원 후 시행한 조영증강 복부CT에서 10cm 크기의 혈종과 dorsal pancreatic artery의 거짓동맥류가 있음. 또한 초기 동맥기 사진에서 상장간막 정맥과 문맥이 조영되는 동정맥루(arteriovenous fistula)가 확인됨 (Fig. 1).
Fig. 1
Coronal reconstruction image of arterial phase CT scan shows a large hematoma and pseudoaneurysm (white arrow) from the dorsal pancreatic artery (arrowhead). Portal vein is strongly enhanced due to arteriomesenteric fistula on arterial phase CT scan (black arrow).
시술방법 및 재료
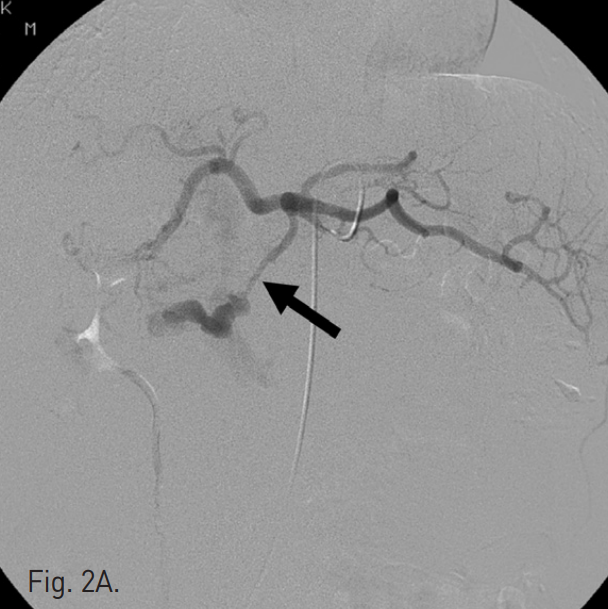
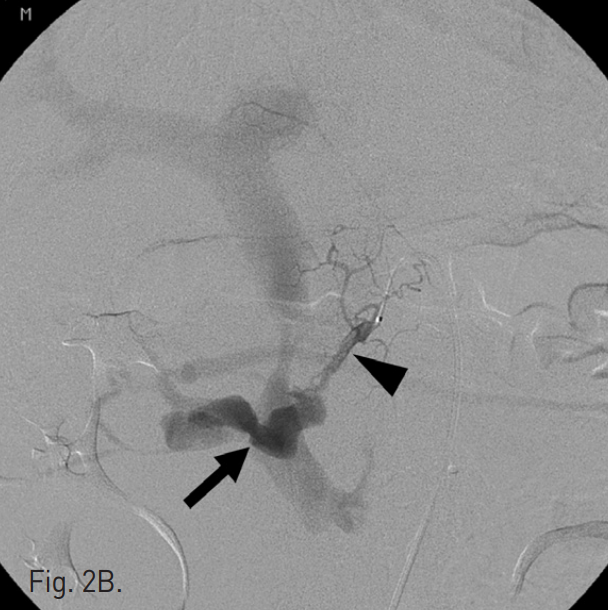
초음파 및 투시 하에서 우측 대퇴동맥을 천자하고 5F Cobra catheter(Cook, Bloomington, IN, USA)를 이용하여 복강동맥 및 상장간막동맥 조영술을 시행하였다. 복강동맥 조영술에서 dorsal pancreatic artery에서 유출되는 조영제의 누출과 거짓동맥류를 확인하였고 상장간막 정맥으로의 동정맥루를 확인하였다(Fig. 2A, B). Microcatheter(Renegade, Boston Scientific, Natick, MA, USA)를 이용하여 이 거짓동맥류를 선택하였고, 10mm Interlock coil(Boston Scientific, Natick, MA, USA) 6개와, 10mm Nester coil(Cook, Bloomington, IN, USA) 3개를 사용하여 embolization을 시행하였다(Fig. 2C). 이후 남아있는 거짓동맥류와 동정맥루에 대하여 NBCA와 lipiodol mixture(3:1)를 이용하여 색전술을 시행하였다. 시술 후 동맥조영술에서 남아있는 거짓동맥류나 상장간막 정맥으로의 동정맥루는 보이지 않았다(Fig. 2D).
Fig. 2
A. Celiac angiography shows a pseudoaneurysm of dorsal pancreatic artery (arrow).
B. Seective angiography of dorsal pancreatic artery (arrow head) shows pseudoaneurysm and arteriovenous fistula to superior mesenteric vein. Por tal vein is visualized erly due to fistulation (arrow).
C. Multiple coil deployment was performed but the arteriovenous fistula is still remained.
D. Celiac angiography after glue embolization shows no residual fistula and pseudoaneurysm.
고찰
췌장동맥의 출혈은 외상, 췌장 및 십이지장 관련 수술환자, 췌장염환자 등에서 종종 발생할 수 있다 [1,2]. 하지만 췌장염 뒤에 발생한 출혈과 이에 동반된 문맥이나 상장간막 정맥으로의 동정맥루 형성은 매우 드물다 [3]. 그러나 이러한 출혈을 보인 환자의 mortality가 20~50%로 높게 보고 되고 있어 빠른 치료가 필요하며 endovascular treatment가 treatment of choice로 여겨진다[4]. 간동맥 또는 위십이지장동맥에 발생한 거짓동맥류 또는 동정맥루는 coil, glue, stent graft등을 이용하여 치료하게 되는데, stent-graft를 이용한 치료가 어려운 경우는 거짓동맥류의 원위부와 근위부 동맥을 모두 차단하여야 효과적으로 치료할 수 있다. 본 증례는 췌장염환자에서 발생한 dorsal pancreatic artery의 거짓동맥류와 상장간막 정맥으로의 동정맥루 증례로 여러 개의 coil과 glue (NBCA)를 이용하여 효과적으로 치료하였다.
참고문헌
1. Shankar S, Russell RC. Haemorrhage in pancreatic disease. Br J Surg 1989; 76(8):863-866.
2. Tessier DJ, Stone WM, Fowl RJ, et al. Clinical features and management of splenic artery pseudoaneurysm: case series and cumulative review of literature. J Vasc Surg 2003; 38(5):969-974.
3. Denys A, Hammel P, de Baere T, et al. Arterioportal fistula due to a ruptured pancreatic pseudocyst: diagnosis and endovascular treament. Am J Roentgenol 1998; 170(5):1205-1206.
4. Krishan S, McPherson S, Pine J, Hayden J. Current Management of Mesenteric Extrahepatic Arterioportal Fisulas: Report of a Case Treated With a Gastroduodenal Artery Stent Graft and Literature Review Vasc Endovascular Surg 2010; 44(2):139-45.
Citations
Citations to this article as recorded by