중심단어
Uterine didelphys, angiography, uterine artery embolization
임상소견
환자는 1달 전부터 계속적인 질 출혈, 부정자궁출혈이 있어 병원에 내원하였다. 환자는 결혼한 상태로 향후 임신계획이 있었고, 과거에 임신이나 유산한 경험은 없었으며, 1년 전부터 발생된 생리기간 중 월경과다 및 심한 생리통을 호소하였다.
영상소견
MR영상에서 두 개의 분리된 완전한 자궁과 자궁경관을 가지는 중복자궁(uterine didelphys) 소견을 보였다. 좌측 자궁에 국소형 자궁선근증이 있었고, 우측자궁은 정상 소견이었다(Fig. 1).
Fig. 1. A 38-year-old woman with uterine didelphys.
T2 weighted coronal MR image shows two separated uteruses and focal adenomyosis (arrows) in left-sided uterus.
시술소견
초음파 유도하에 우측 대퇴동맥을 천자하여 5F sheath(Terumo, Tokyo, Japan)를 삽입하였다. Pigtail 카테터(Cook, Bloonington, IN, USA)를 하부 대동맥에 위치시킨 후 골반조영술을 시행한 결과, 좌측 자궁동맥의 비대가 관찰되었다(Fig. 2a). 양측 자궁은 각각의 자궁 동맥으로부터 영양 공급을 받고 있었으며 두 동맥은 거의 서로 연결되어 있지 않았고 완전히 독림된 자궁이 조영되었다(Fig. 2b). 5 F Cobra 카테터(Cook, Bloonington, IN, USA)로 좌측 내장골동맥에 진입시키고 Microferret 카테터(Cook, Bloonington, IN, USA)로 좌측 자궁동맥을 선택하였다. 자궁동맥의 상행분절에 Microferret 카테터를 위치시키고 polyvinyl alcohol(PVA)(Contour, Bostonscientific, Fremint. Calif)을 이용하여 자궁동맥 색전술을 시행하였다. 150-250 micrometer, 250-355 micrometer, 355-500 micrometer의 PVA를 순서대로 사용하는 1-2-3 프로토콜로 색전술을 시행하였다. 이때 조영제와 식염수가 1:1로 섞인 용액에 PVA입자를 넣어서 총 60ml를 만들었는데, 각각의 사용한 양은 20cc( 1/3 vial), 40cc(2/3 vial), 20cc(1/3 vial) 이었다. 10 번의 심장박동 동안 자궁 동맥내에 조영제의 정체가 보일 때까지 색전술을 시행하였다. 우측 자궁동맥 조영술에서 좌측 자궁과 연결 되는 작은혈관이 관찰 되었으나 향후 체외수정을 고려하여 색전술을 시행하지 않았다(Fig. 3). 색전술 후 3개월째 시행한 MR에서 선근증 완전괴사를 관찰할 수 있었으며 좌측 자궁은 44.3%의 볼륨감소를 보였다(Fig. 4a-b). 시
술 전 증상을 10점으로 가정했을 때 생리양의 경우 10점에서 5점, 생리통은 10점에서 0점으로 감소하였다.
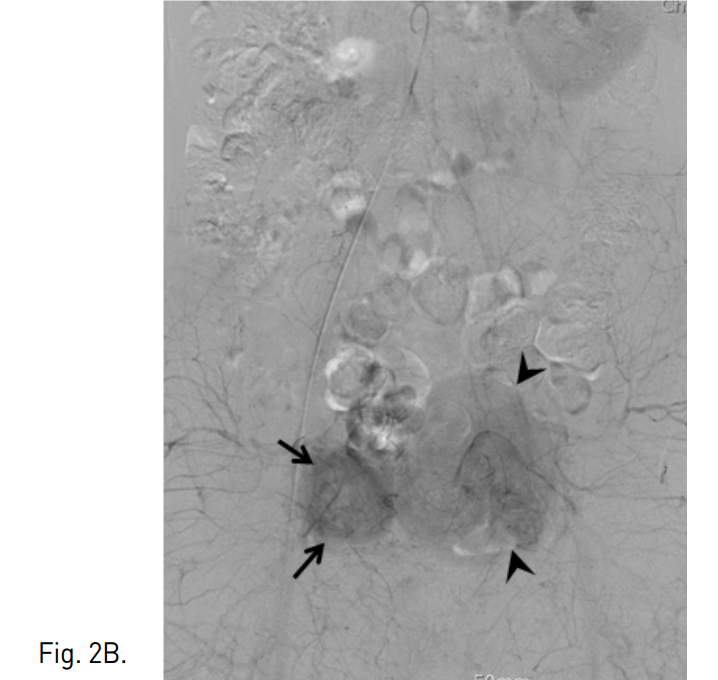
Fig. 2
A, B. Pelvic aortogram shows tortous and dilated left uterine artery (arrow) and two separated uteruses (arrows and arrowheads in B).
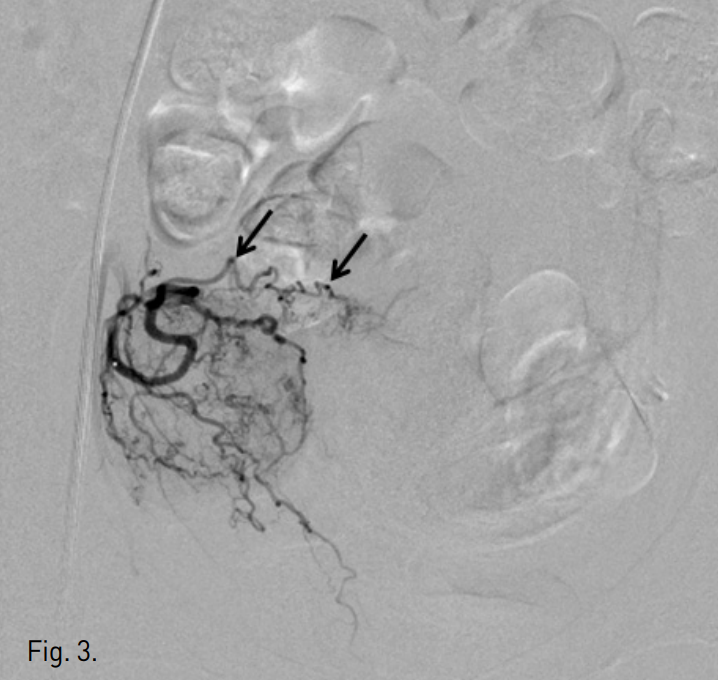
Fig. 3
The right uterine arteriogram demonstrates small branch (arrows) outside the right-sided uterus communicating with the left-sided uterus.
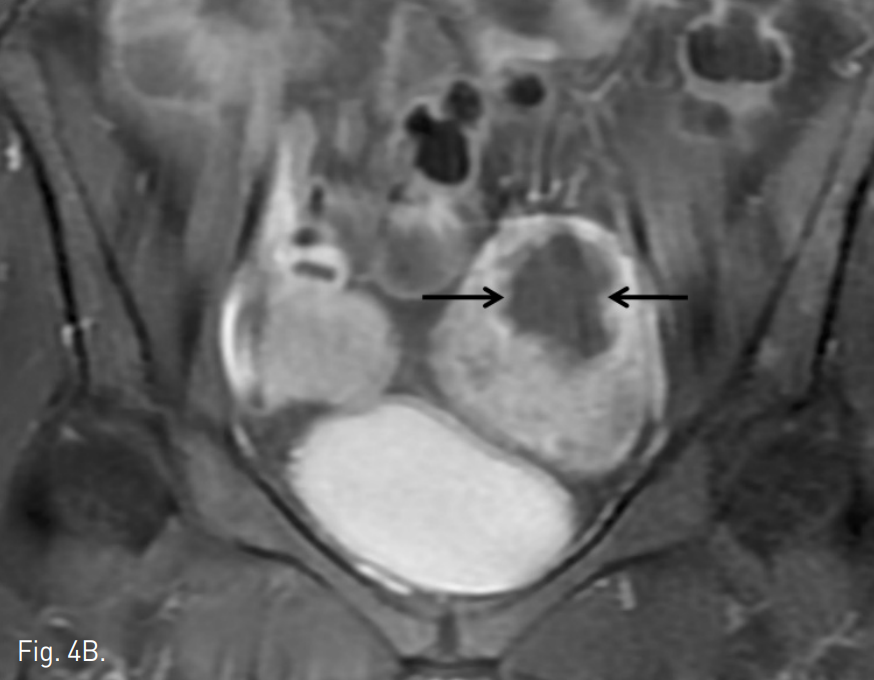
Fig. 4
A, B. T2 weighted (A) and contrast enhanced (B) MR images taken three months after embolization show 44% volume reduction of the left-sided uterus and non-perfusion area in adenomyosis (arrows in A and B).
고찰
자궁기형의 빈도는 전체 일반인 중 0.5%이며 이 중에서 중복 자궁은 약 11%정도를 차지하는 비교적 드문 기형이다(1). 발생학적으로 두개의 뮐러관이 완전히 융합하는데 실패하여 생기는 자궁 기형으로, 두 개의 자궁이 완벽하게 분리되어 있고 각각의 자궁경부를 가진다. 중복자궁은 두 개의 분리된 자궁이 정상 zonal anatomy를 가진다. 하지만 이러한 환자에서 자궁동맥 혈관조영술 소견은 아직 보고가 없다. 본 증례에서는 중복자궁은 각각 동측의 자궁 동맥으로부터 거의 독립적으로 영양공급을 받음을 알 수 있었고 다만 매우 작은 혈관이 연결되어 있었다. 자궁선근증의 빈도는 10-18% 정도이며 가장 흔한 증상은 비정상 자궁출혈과 월경통이며 그 외에도 골반의 묵직함, 빈뇨 등의 증상이 있다(2). 자궁선근증의 완전한 치료를 위해서는 자궁절
제술이 권유되고 있으나 최근에 자궁동맥 색전술이 자궁선근증의 대체적인 치료방법으로 제시되고 있다(3). 치료의 효과 면에 있어서 아직 논란의 여지가 되고 있으며 좀더 장기적인 효과에 관해서는 추가적인 연구가 필요하다(2, 4, 5). 특히 사용한 PVA입자의 크기에 따라 다양하게 결과가 보고되고 있다.
최근 김(6) 등은 PVA 입자를 크기별로 순서대로 사용하는 1-2-3 프로토콜 방법이 소개되었고 전체 환자의 82.5%의 환자에서 선근종의 완전괴사를 보고하였다.
따라서 본 증례의 경우에도 김 등이 제시한 1-2-3 protocol을 따라 자궁 동맥 색전술을 시행하였고 세 달 후 추적검사에서 자궁선근증의 완전괴사를 보였다.
본 증례는 드문 자궁기형의 한 종류인 중복자궁을 가진 환자에서의 자궁동맥 혈관 조영술 소견과 이와 동반되어 한쪽 자궁에서 발생한 선근증을 자궁동맥색전술로 성공적인 치료하였다는데 의의가 있으며 계속적인 추적관찰을 통해 장기적인 치료효과를 판단하는 것이 필요할 것으로 생각된다.
참고문헌
1. Nahum GG. Uterine anomalies. How common are they, and what is their distribution among subtypes? J Reprod Med 1998; 43:877-887.
2. Englander MJ. Uterine artery embolization for the treatment of adenomyosis. Semin Intervent Radid 2008;25:387-393.
3. Levgur M. Therapeutic options for adenomyosis: a review. Arch Gynecol Obstet 2007; 276:1-15.
4. Pelage JP, Jacob D, Fazel A, Namur J, Laurent A, Rymer R, et al. Midterm results of uterine artery embolizafon for symptomatic adenomyosis initial experience. Radiology 2005; 234:948-953.
5. Kim MD, Kim S, Kim NK Lee MH, Ahn EH, Kim HJ, et al. Long-term results of uterine artery embolization for symptomatic adenomyosis. AJR Am J Roentgend 2007;188:176-181.
6. Kim MD, Kim YM, Kim HC, Cho JH, Kang HG, Lee C, et al. Uterine Artery Embolization for Symptomatic Adenomyosis A New Technical Development of the 1-2-3 Protocol and Predictive Factors of MR Imaging Affecting Outcomes. J Vasc Interv Radiol 2011; 44:497-502.
Citations
Citations to this article as recorded by