중심단어
Pancreatitis, Portalvein, Stenosis, Stent
임상소견
지난 5년간 반복적인 췌장염이 있었던 환자로 췌장경부에 있는 가성낭종에대한 검사를 하는 도중 주문맥의 심한 협착이 발견되어 식도 및 위정맥류의 발생을 예방하기 위하여 문맥 협착에 대한 ste nt 삽입술이 의뢰됨.
진단명
Chronic pancreatitis with portal vein stenosis
영상소견
조영증강 복부 CT에서 췌장 경부 상부에 침윤성의 연부조직 음영이 보이며 3cm 정도 크기의 낭성병변이 동반되어 있음. 주문맥은 상기한 연부조직 음영으로 둘러싸여 있고 협착이 있음.주문맥 주위로 해면상변환 (cavernous transformation)이 보임(Fig 1).
Fig. 1
A-B. On CT, soft tissue densities are infiltrated around main portal vein and pancreas. Portal vein (arrow in A) is narrowed and many small collateral vessels (double arrow in B) are around main portal vein. There is about 3cm sized cystic mass close to infiltrative soft tissue densities (arrowhead in A).
시술방법 및 재료
21G Chiba needle을 이용하여 경피적으로우간문맥(P6)을 천자한 후 0.035"guidewire (Guide wire M, Terumo, Tokyo, Japan)를 이용하여 5F catheter (Soft Vu, AngioDynamics, Queensbury, NY)를 주간문맥에 위치시킨 후 문맥조영술을 시행하였음. 주문맥에 4~5cm의 심한 협착(90%)이 있으며 주문맥 주변으로 해면상 변환 (cavernous transformation)에 의한 곁순환 혈관(collateral vessel)이 보임. 협착 원위부의 문맥압은 26mmHg, 위창자간막정맥(supsuperior mesenteric vein, SMV)과 비장정맥(splenic vein)의 압력은 17mmHg로 협착 근위부와 원위부의압력차는 9mmHg임(Fig 2A).
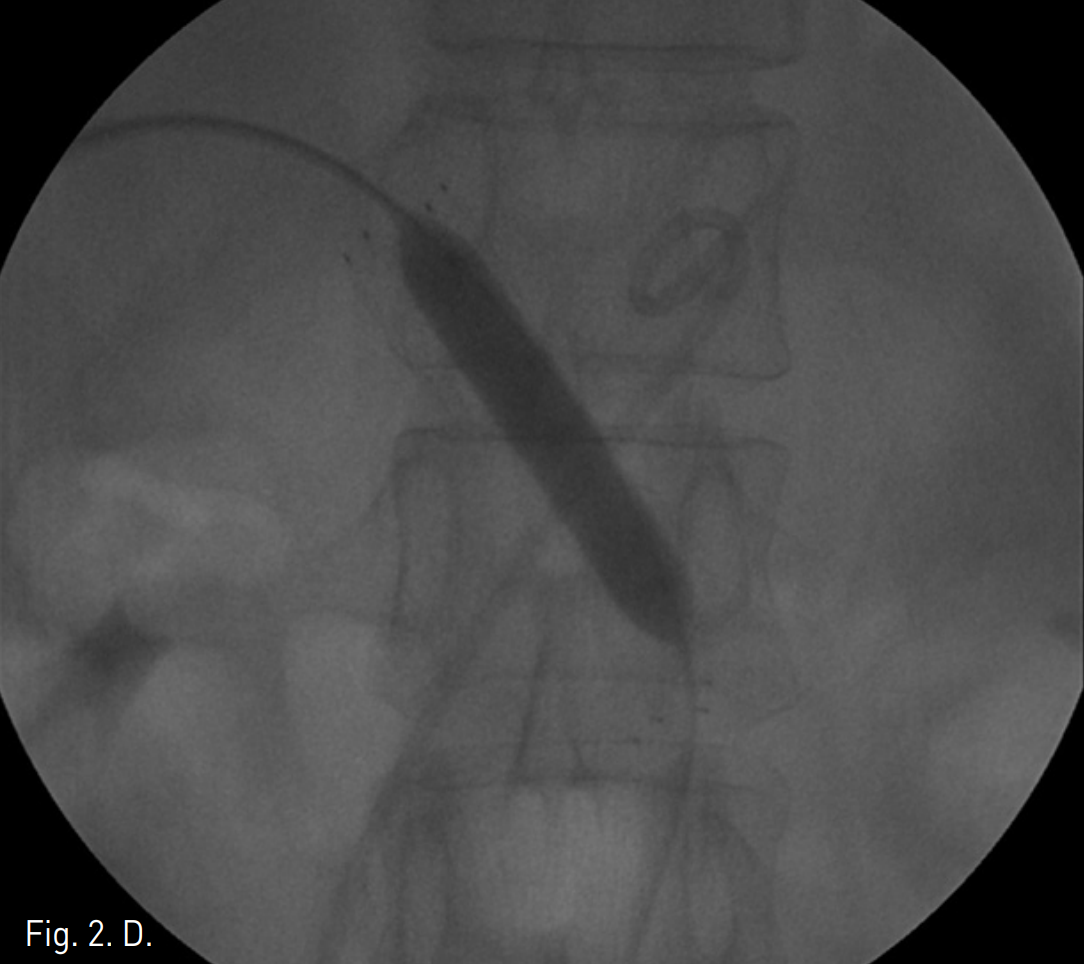
주문맥의 협착부위에서 10mm x 4cm balloon catheter (Synergy, Boston Scientific, Natick, Mass)를 사용하여 풍선확장술을 시행하였으나 elastic recoil로 인하여 반응이 없었음(Fig 2B-C). 자가팽창스텐트(14mm, 6cm, Zilver, Cook, USA)를 협착부위에 설치하고 10mm x 4cm balloon(Synergy, Boston Scientific, Natick, Mass)을 이용하여 post-stent balloon dilatation을 시행함. (Fig 2D)Stent 설치 후 협착 근위부와 원위부의 압력차는 1mmHg (SMV는 18mmHg, 주간문맥은 17mmHg)로 감소되었음(Fig 2E).
간문맥 천자에 사용된 경로는 N-butyl-Cyanoacrylate를 이용하여 막음.
Fig. 2
A. P6 is punctured by a 21G needle percutaneously and catheter is introduced into main portal vein. On portogram, thereis a short segmen talpor tal stenosis of 4~5cm in length and many small collateral vessels around main portal vein as cavernous transformation. Pressure gradient is 9 mmHg. (portal vein; 26mmHg, SMV and splenic vein; 17mmHg).
B. Balloon dilatation for portal vein stenosis is performed.
C. After balloon dilatation, portal vein stenosis is still present.
D. Stentis placed in portal vein and post balloon dilatation is performed.
E. After stent placement, portal stenosis is disappeared on portogram and pressure gradient between portal vein and SMV is decr eased to 1 mmHg. Also, visible collateral vessels are markedly decreased.
고찰
Symptomatic prehepatic portal hypertension의 가장 흔한 원인은 문맥혈 전증 (portal vein thrombosis)이며 extensive abdominal infection이나 abscess 같은 다양한 원인에 의하여 발생할 수 있다(1). 그 외에도 간이식이나 간절제술후 late complication으로(2) 또는 췌장암(pancreatic cancer)이나 간암(hepatocellular car cinoma)(3-5)에 의하여 문맥 협착(portal vein stenosis)이 발생할 수 있다.
만성 췌장염이나 중증의 급성 췌장염 환자에서 splanchnic venous involement는 잘 알려진 합병증이며 비장정맥(splenic vein)이 가장 흔히 침범되며 위창자간막 정맥(superior mesenteric vein)이나 간문맥(portal vein) 역시 침범될 수 있다(6). 이러한 췌장염에 의한 문맥폐쇄(portal vein obstruction)는 대부분 혈전성 폐색 (thrombotic occlusion)에 의하며 국소협착(focal stenosis)은 드물다고 알려져있다(1). 만성췌장염에서 간문맥의 국소협착은 지속적인 염증, 흉터형성, 또는 가성낭종에 의한 압박에 의하여 발생하는 것으로 추정된다(6).
본례에서는 문맥고혈압에 의한 증상은 없었지만 몇몇 보고된 증례에서는 여러 원인에 의한 문맥협착에서 refractory ascites, jejunalvariceal bleeding, gastroesophagea lvarix, hematemesis, melena 같은 증상이 보고되어 있으며 문맥협착이 직경의 80% 이상 일때 문맥고혈압의 증상이 나타나고 간기능부전이 발생하지만 50% 미만에서는 증상이 없다는 보고도 있다(1, 7-8), 치료로는 medical conservative treatment나 surgical shunt creation이 있지만 결과가 좋지 않으며 operative morbidity 와 mortality가 높다. Percutaneous transhepatic portal venous stent placement는 복강내 출혈이나 담도손상 같은 합병증이 있을 수 있지만 Shan, et al. 은 6례의 percutaneous transhepatic portal venous stent placement 후 abdominal pain, transient fever 같은 minor complication은 있었지만 severe complication은 없었다고 보고하였다(8). 국소적 문맥협착에 대한 balloon dilatation은 대부분 elastic recoil에 의하여 효과가 없었고 stent placement를 시행하였을 때 증상소실 및 collateral vessel의 소실을 즉시 관찰할 수 있었다(1, 6-8). Funaki 등은 12례의 문맥내 스텐트삽입술(portal venous stent place ment) 후 4년 가까이 추적관찰하였을 때 further intervention이 필요한 경우는 없었다고 보고하였다(9).
국소적 문맥협착에 대한 percutaneous transhe patic portal venous stent placement는 비교적 안전하면서 치료효과가 우수한 시술로 생각된다.
References
1. G. Maleux, J. Vaninbroukx, C. Verslype, et al. Pancreatiis-induced extrahepatic portal vein stenosis treated by percutaneous transhepatic stent placement. Cardio vascInterventRadiol 2003; 26:395-397.
2. Funaki B, Rosenblum JD, Leef JA, et al. Portal vein stenosis in children with segmental lver transplants: Treatment with percutaneous transhepaticvenoplasty. AJR 1995; 165:161-165.
3. Mathias K, Bolder U, Lo hlein D, Ja ger H Percutaneous transhepatic angioplasty and stent implantation for prehepatic portal vein obstruction. CardiovascInterventRadiol 1993; 16:313-315.
4. Yamakado K, Nakatsuka A, Tanaka N, et al. Malignant portal venous obstructions treated by stent placement:Significant factors affecting patency. J VascInterventRadiol 2001; 12:1407-1415.
5. Yamakado K, Tanaka N, Nakatsuka A et al. Clinical efficacy of portal vein stent placement in patients with hepatocellular carcinoma invading the main portal vein. J Hepatol 1999; 30660-668.
6. Schaible R, Textor J, Decker P, et al. Transjugular portal venous stenting in inflammatory extrahepatic portal vein stenosis. CardiovascInterventRadiol 2002;25:530-532.
7. Hiraoka K, Kondo S, Ambo Y, et al. Portal venous dilatation and stenting for bleeding jejunalvarices : Report of two cases. Surg Today 2001; 31:1008-1011.
8. Shan H, Xiao XS, Huang MS, et al. Portal venous stent placement for treatment of portal hypertension caused by benign main portal vein stenosis. World J Gastroenterol 2005; 1:3315-3318
9. Funaki B, Rosenblum JD, Leef JA, et al. Percutaneous treatment of portal venous stenosis in children and adolescents with segmental hepatic transpants: Long term results. Radiology 2000; 215:147-151.
Citations
Citations to this article as recorded by