중심단어
Liver transplantation, Hepatic vein, Metallic stent
임상소견
만성 B형 간염 환자로 간경변증 진단 받고 외래 통원치료 하던 중 간성뇌병증 등으로 수 차례 입원 반복하여 생체장기제공자 간이식술(Living donor liver transplantation, LDLT)을 받았다. 수술 전 평가 중 발견된 splenorenal shunt에 대해 코일색전술을 시행한 상태였다. 공여자는 수혜자의 자녀로서 38세 여성이었다.
영상소견
수술 후 1일 째 시행한 color doppler 검사에서 오른간 정맥의 spectral waveform이 monophasic하여 hepatic outflow의 장애가 의심되었다. Liver CT에서 오른간정맥의 기시부가 좁아져 있었으며(Fig. 1) 인접한 아래대정맥 내에 소량의 혈전이 의심되었다. 정맥조영술을 시행하였으며 오른간정맥과 아래대정맥 사이의 관강내(intraluminal) 협착 소견을 확인할 수 있었다(Fig. 2).
Fig. 1
Contrast-enhanced CT scan shows a focal stenosis at right hepatic vein-IVC anastomosis (arrow).
Fig. 2
Right hepatic venogram shows a filling defect of the right hepatic vein-IVC anastomotic site (arrow).
시술방법 및 재료
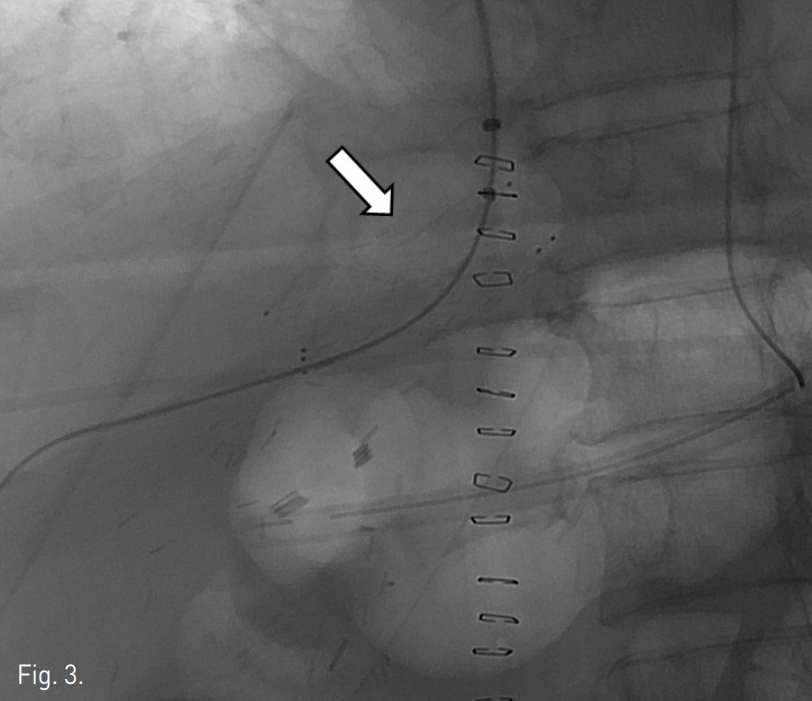
오른손목정맥을 천자한 뒤 6F shuttle sheath (Cook, Bloomington, U.S.A)를 삽입하였다. Cobra catheter (Cook, Bloomington, U.S.A)와 0.035-유도철사 (Terumo, Japan)를 이용해 오른간정맥을 선택한 후 협착된 부위를 사이에 두고 원위부 간정맥과 아래대정맥 간 측정한 pressure gradient는 9~10mmHg였다. 협착된 부위에 14mm x 4cm
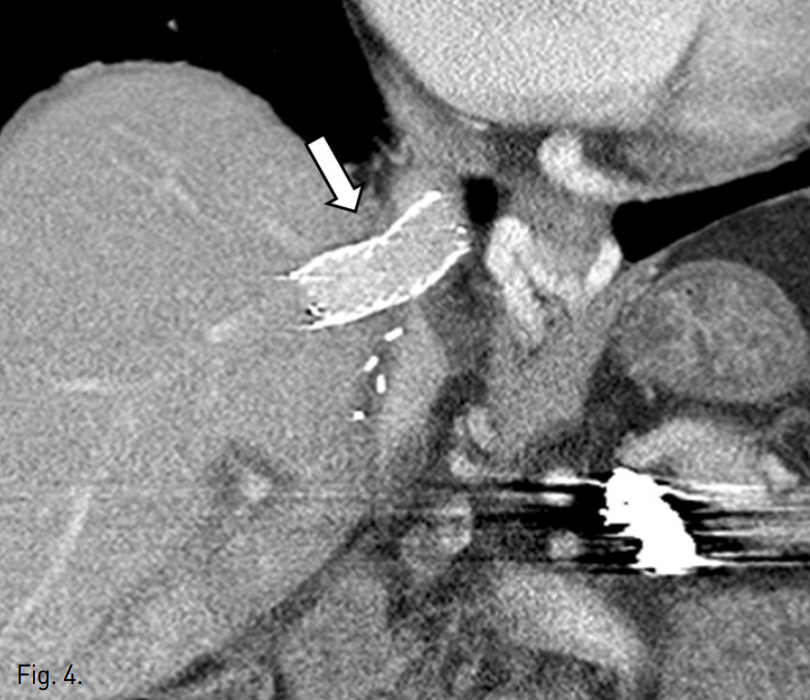
Zilver 스텐트 (Cook, Bloomington, U.S.A)를 삽입하였다(Fig. 3). 스텐트 삽입 후 측정한 pressure gradient는 4mmHg로 감소되었으며 정맥조영술에서 협착은 보이지 않았다. 시술 직후 통증이나 활력 징후의 변화와 같은 합병증은 관찰되지 않았다. 시술 다음날 시행한 color doppler 검사에서 오른간정맥의 spectral waveform이 triphasic하게 관찰되었으며 추적 검사에서도 동일한 소견이 관찰되었다. 시술 후 시행한 CT angiography에서 스텐트는 이전 CT에서 보였던 협착된 부위에 삽입되어 있음을 확인하였고, 스텐
트 내부의 혈전 또는 꼬임 등 이상소견은 보이지 않았다(Fig. 4). 환자는 보존적 치료 후 퇴원하였다.
Fig. 3
A self expandable metallic stent (arrow) was successfully placed across the anastomotic stenosis.
Fig. 4
Follow-up CT scan shows widely patent stent lumen (arrow).
고찰
간이식술 후 발생하는 hepatic outflow obstruction은 드물지만 복수나 간기능이상 등을 일으킬 수 있는 중요한 합병증이다. 보통 수술 이후 시행하는 color doppler 검사에서 monophasic pattern을 보이거나, 복수나 부종 등의 증상이 나타날 때 hepatic outflow obstruction을 의심하게 된다. 오른심방과 간정맥 사이의 venous pressure gradient가 3mmHg 이상일 경우, 협착 전 후 pressure gradient가 5mmHg 이상이면 치료의 적응증이 된다. 같은자리간이식술 (Orthotopic liver transplantation, OLT) 후의 hepatic outflow obstruction 발생률은 1%정도이지만 LDLT 후의 발생률은 2~4% 정도로 보고되고 있다. OLT 시에는 장기제공자의 아래대정맥의 일부를 간과 함께 절제하여 문합하지만, LDLT 시에는 장기제공자의 간정맥을 받는 이의 간정맥 또는 아래대정맥과 문합해야 하므로 문합 부위의 직경이 좁아 hepatic outflow obstruction이 더 흔하다. 또한 LDLT의 경우 이식한 간이 자라나면서 hepatic outflow tract이 당겨지거나 꼬이면서 폐색이 발생할 수도 있다고 알려져 있다. 일반적으로 수술 직후 발생한 hepatic outflow obstruction의 경우 응급 재수술의 적응증이 되고, late-onset인 경우는 문합부위의 fibrotic change로 인해 재수술이 어려워 경피적 치료의 적응증이 된다. 그러나 수술 후 수일 내 발생한 hepatic outflow obstruction에서 응급 재수술이 경피적 치료에 비해 우월하다는 연구 결과는 아직 없다. 경피적 치료는 응급 재수술에 비해 시술 시간이 짧고 출혈량이 적으며 전신마취가 필요 없다는 장점을 가지고 있다. 그러나 수술 후 수일 내에는 문합부위의 조직이 치유되지 않은 상태이므로 경피적 치료 시 문합부위의 파열 등이 발생할 가능성이 있으며, 조영제에 의한 부작용도 발생할 수 있으므로 이와 관련하여 응급 재수술과 경피적 치료의 결과를 비교한 연구가 필요하리라 생각된다.
References
1. Kubo T, Shibata T, Itoh K, et al. Outcome of Percutaneous Transhepatic Venoplasty for Hepatic Venous outflow Obstruction after Living Donor Liver
Transplantation. Radiology 2006;239:285-290.
2. Ikeda 0, Tamura Y, Nakasone Y, et al. Percutaneous transluminal venoplasty after venous pressure measurement in patients with hepatic venous outflow obstruction after living donor liver transplantation. Jp J Radiol 2010; 28:520-526.
3. Cheng YF, Chen CL, Huang TL, et al. Angioplasty treatment of hepatic vein stenosis in pediatric liver transplants: long-term results. Transplant International 2005; 18:556-561.
4. Tanimoto Y, Tashiro H, Itamoto T, et al. Hepatic venous outflow obstruction after right lateral sector living-donor liver transplantation, treated by insertion of an expandable metallic stent. J Hepatobiliary Pancreat Surg 2008; 15:228-231.
Citations
Citations to this article as recorded by