중심단어
subclavian artery, thromboembolism, protection device
임상소견
내원 3일 전부터 발생한 왼팔의 얼얼한 느낌과 통증. 내원 후 시행한 심초음파에서 Moderate mitral stenosis with left atrial enlargement 확인.
영상소견
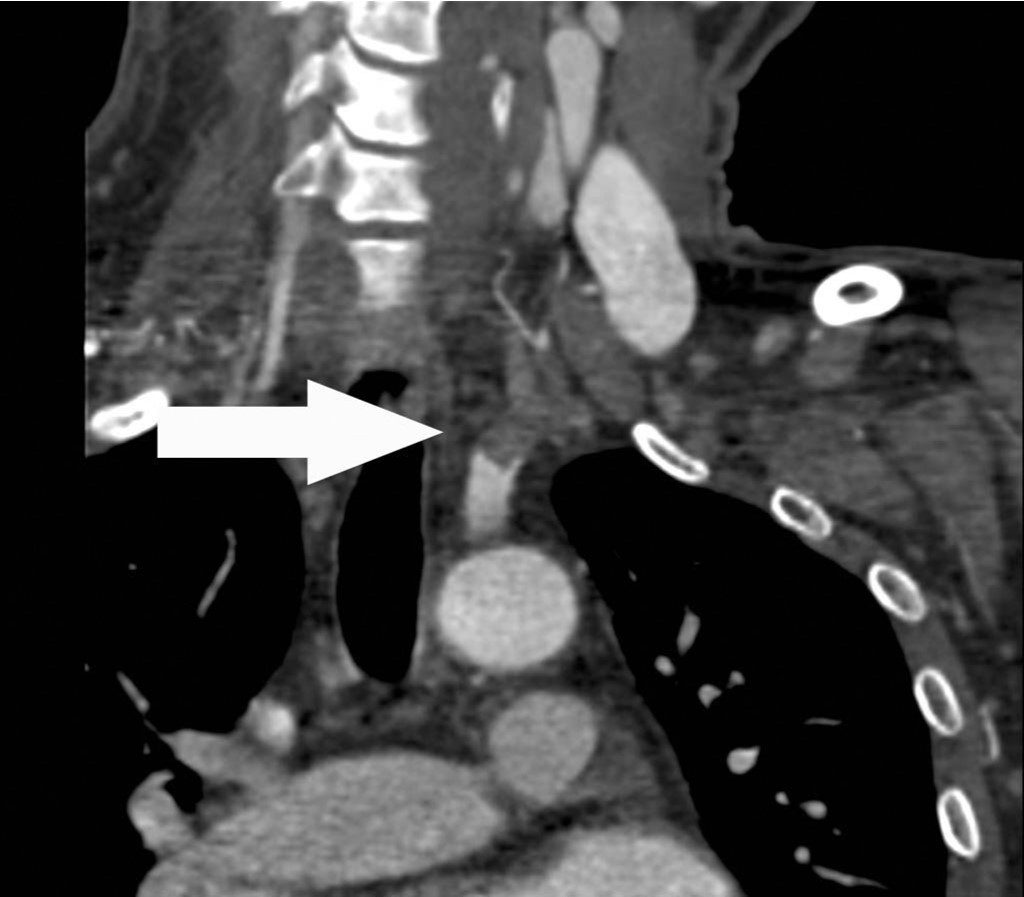
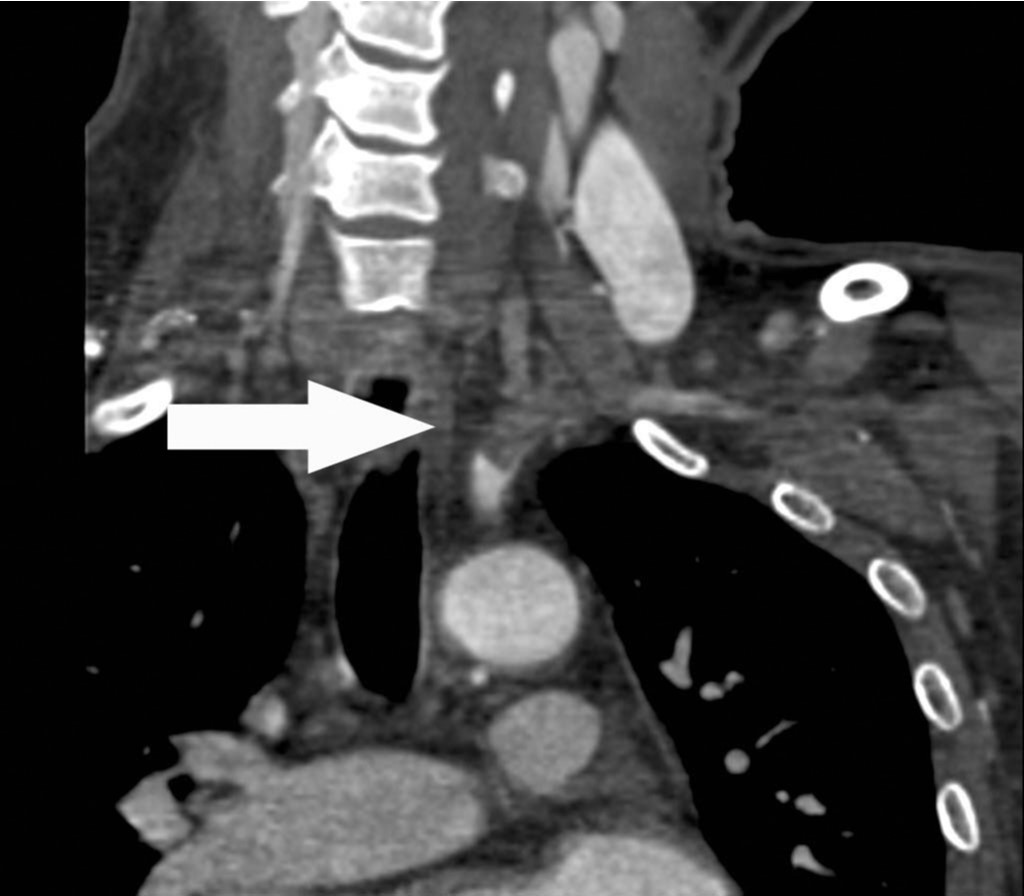
상지 CT 혈관조영술 관상면 영상에서 좌측 쇄골하동맥의 근위부에서 약 7cm에 걸쳐 혈전색전증에 의한 혈관의 부분폐쇄가 확인되고(Fig. 1A, B, C), 혈전색전증은 좌측 추골동맥 근위부로도 연장되어 있음(Fig. 1D).
Fig. 1. A-D
Fig. 1A-D Coronal CT images show a partial thrombotic occlusion at proximal subclavian artery (SCA, arrow in Fig. 1A-C), and proximal vertebral artery (VA, arrow head in Fig. 1D).
시술방법 및 재료
우측 총대퇴동맥을 통해 6Fr sheath (Terumo,Tokyo, Japan)를 거치 후 5Fr head hunter catheter(Cook, Bloomington, IN, USA)로 좌측 쇄골하동맥조영술을 시행하였음. 혈관조영 영상에서 좌측 쇄골하동맥 근위부에서 7cm에 걸쳐 혈전색전증에 의한 충만 결손이 확인되었고 이로 인해 좌측 쇄골하동맥은 부분 폐쇄 소견을 보였음. 혈전색전증은 동측 추골동맥 근위부로도 연장되어 충만결손으로 확인되고 있음(Fig. 2). 이 상태에서 기계적 혈전제거술이나 혈전용해술을 시행할 경우 추골동맥 색전증 발생위험이 있어 필터형 원위부 색전보호기구를 사용하여 시술을 시행하기로 하고 6Fr guiding catheter (Envoy, Cordis, FL, USA)를 좌측 쇄골하동맥 기시부에 위치시킨 후 0.014inch 205cm microwire (Transend EX soft tip, Boston scientific, FL, USA)를 좌측 추골동맥에 거치하였음. Wire를 따라 필터 크기가 5mm인 원위부 색전보호기구(SpiderFX™ Embolic Protection Device, ev3, MN, USA)를 V2 segment에 설치하였음(Fig. 3). 이후 초음파 유도 하에 micropuncture set (Enpath Medical, MN, USA)를 사용하여 좌측 상완동맥을 접근하여 7Fr sheath (Terumo, Tokyo, Japan)를 거치 후 7Fr guiding catheter (Guider soft tip, Boston scientific, MA, USA)를 사용하여 수 차례 혈전흡입술을 시행하였음. 다량의 혈전을 흡입제거한 후 시행한 좌측 쇄골하동맥 조영술상 남은 혈전은 추골동맥기시부보다 원위부 쇄골하동맥에 위치하고 있고 시술 중 추골동맥 원위부로 이동한 혈전은 모두 원위부 색전보호기구에 포착되어 충만결손으로 확인되었음(Fig. 4). 원위부 색전보호기구를 partial enclosure recovery기법으로 회수하였고, 이후 시행한 좌측 쇄골하동맥조영술상 추골동맥은 이상소견이 없었고 뇌후순환계에도 색전 합병증은 발생하지 않았음. 추골동맥 기시부보다 원위부 쇄골하동맥에 위치한 혈전색전증은 혈전용해술이 가능하여 5Fr multipurpose catheterr (Cook, Bloomington, IN, USA)를 혈전 중간부위에 거치 후 12시간 동안 유로카이네이스 지속투여(60000unit/h)를, 좌측 상완동맥에 거치한 7Fr sheath로는 헤파린 지속투여(500unit/h)를 시행하였음. 12시간 경과 후 시행한 좌측 쇄골하동맥조영술 상 일부 벽혈전이 남아 한차례 더 혈전을 흡입제거 하였고, 남아있는 혈전 없이 좌측 쇄골하동맥이 개통된 것을 확인 후 시술을 마쳤음(Fig. 5).
Fig. 2
Left subclavian artery angiogram shows a partial arterial filling defects in proximal SCA and VA (arrow).
Fig. 3
A 5mm diameter distal embolic protection device (arrow) was placed in the V2 segment.
Fig. 4
Immediate after catheter suction thromboembolectomy, SCA angiogram shows some filtered embolus at distal embolic protection device (arrow).
Fig. 5
Final angiogram shows a patent SCA without residual thromboembolus.
고찰
급성사지허혈(acute limb ischemia, ALI)은 사지관류의 갑작스런 감소를 초래하는 원인에 의해 limb viability가 위협받는 상태로 14일 미만의 경과를 보일 때를 말한다. 원인은 다양하나 atherosclerosis에 의한 thrombosis in situ와 embolism이 가장 흔하고, 그 외 dissection, intimal hyperplasia, hypercoa gulable state, trauma, vasculitis, aneurysm thrombosis등의 원인이 있다. 이 중 Embolism은 심장, 동맥류, 근위부 동맥경화반이나 협착에서 기인할 수 있다. 본 증례와 같이 ALI 환자에서 atrial arrhythmia (flutter/fibrillation), congestive heart failure, valvular heart disease가 있는 경우 arterial embolism을 원인으로 의심할 수 있다. ALI의 임상분류는 치료방침을 결정하는데 중요하며 sensory loss, muscle weakness 정도와 peripheral pulses에 대한 Doppler 검사를 종합하여 ALI의 clinical categories를 정할 수 있다. ALI 환자의 clinical category가 I (viable), IIa (marginally threatened)인 경우 치료는 thrombolysis나 surgical treatment (open embolectomy, thrombectomy)가 모두 가능하다. Category IIb (immediately threatened)인 경우에는 revascularized tissue에 bleeding이 발생하여 compartment syndrome이 유발될 수 있어 thrombolysis 보다는 즉시 재관류가 가능한 fogarty embolectomy같은 수술을 권유하고 case-by-case로 thrombolysis를 시행할 수도 있다. 그러나 category III (irreversible)인 경우 early stage에서는 surgical thrombectomy를 고려할 수 있으나 advanced stage에서는 amputation 외에는 방법이 없다.
ALI 환자가 내원하면 즉시 헤파린 정주로 항응고 치료를 시작하고 적응증이 되는 경우 혈전용해 치료(catheter directed therapy)를 하게 된다. 이때 사용하는 혈전용해제로는 urokinase나 tPA 등이 있으며, urokinase의 경우 많이 사용되는 protocol로 graded infusion regimen (240,000U/h x 4h 이후 120,000U/h x maximum 48h)이 있으나 low-dose regimen (50,000U/h)과 효과가 같다는 보고도 있다. 혈전용해 치료 시 catheter suction thrombo embolectomy나 mechanical thromboembolectomy를 같이 시행하면 혈관 개통에 걸리는 시간을 줄일 수 있다. 혈류가 회복되면 혈관조영검사를 통해 혈관구조나 기저병변을 확인하고 적절한 인터벤션이나 수술치료를 추가로 시행할 수 있다.
상지는 하지보다 limb-threatening ischemia가 적고, embous가 원인인 경우가 더 많다. 치료는 전술한 바와 같지만 혈전색전증이 상지혈관 근위부에 위치한 경우 치료 중 총경동맥이나 추골동맥 색전증이 발생할 수 있어 기술적으로 어려울 수 있다. 이 경우 필터형 원위부 색전보호기구가 도움이 되나 1시간 미만으로 설치 사용하여야 하므로 catheter suction thromboembolectomy 시 예방적으로 사용하는 것이 치료에 도움이 된다.
참고문헌
1. Norgren L, Hiatt W, Dormandy J et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg 2007; 45(1):S5A-S65A.
2. Rajan DK, Patel NH, Valji K et al. Quality Improvement Guidelines for Percutaneous Management of Acute Limb Ischemia. J Vasc Interv Radiol 2009; 20:S208-S218.
3. Rutherford RB, Baker JD, Ernst C et al. Recommended standards for reports dealing with lower extremity ischemia: revised version. J Vasc Surg 1997; 26:517- 538.
4. Michael TT, Banerjee S, Brilakis E. Subclavian Artery Intervention with Vertebral Embolic Protection. Catheter Cardiovasc Interv 2009; 74:22-25.
Citations
Citations to this article as recorded by