중심단어
Arteriovenous fistula, transplantation, coil, embolization
임상소견
만성 신부전으로 10개월 전 동종 신장이식을 받고 지내오던 중, 10일 전부터 발생한 우하복부 통증을 주소로 내원하였다.
진단명
AV fistula and hydronephroureterosis with ureter stone in transplanted kidney
영상소견
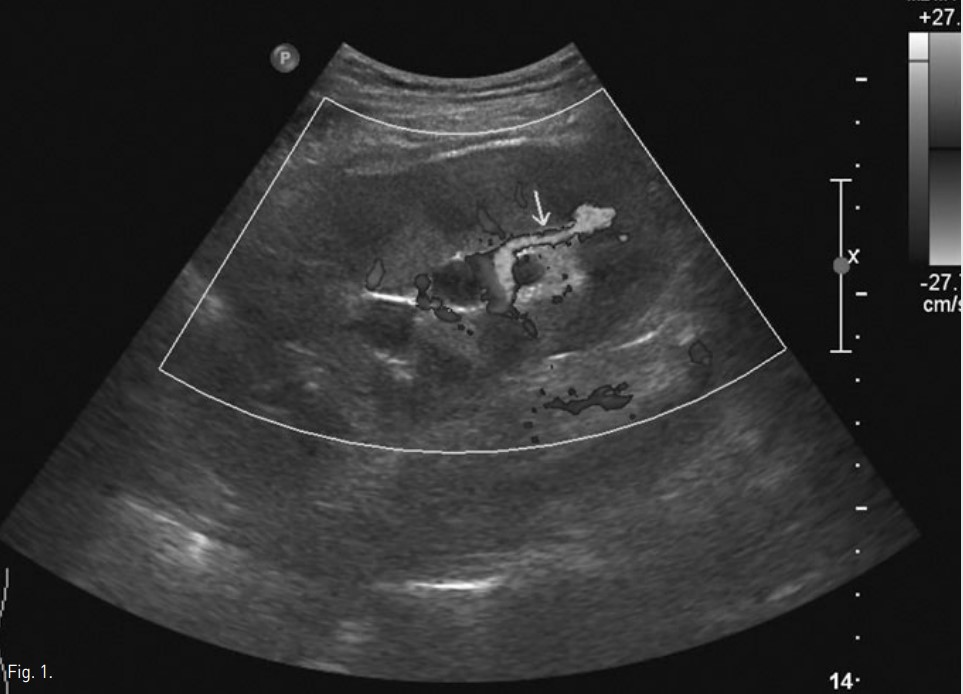
우하복부에 이식된 신장에 대한 초음파 검사상 신우, 신배와 요관의 확장과 함께 요관 원위부에 직경 15mm의 후방 그림자를 동반한 고에코 병변이 관찰되었고, 이는 원위부 요로 결석에 의한 수신증으로 진단되었다. 아울러 color doppler 초음파상 이식신의 하극(lower pole)에 혈액 와류(turbulent blood flow)가 관찰되고 분절동맥과 분절정맥의 연결과 함께 분절동맥 확장이 관찰되어 arteriovenous fistula도 진단되었다.
Fig. 1.
Color Doppler US shows arteriovenous fistula (arrow) in the lower pole of the transplanted kidney.
시술방법 및 재료
좌측 총대퇴동맥을 천자하여 6F sheath를 거치한 후 0.035-inch guidewire(Terumo, Tokyo, Japan)와 5F pigtail catheter(Cook, Bloomington, USA)를 이용하여 골반혈관조영술을 시행하였다. 이를 통해 우측 내장골동맥과 이식신의 신동맥 문합을 확인하였고, 이식신 하극의 분엽동맥(lobar artery)에 연결된 동정맥루를 통해 확장된 신정맥 및 대정맥으로 혈류가 조기 유출되는 것을 확인하였다. 5F Yashiro catheter(Terumo, Tokyo, Japan)를 내장골동맥에 위치시킨 후 2.2F microcatheter(Progreat, Terumo, Tokyo, Japan)와 0.014-inch guidewire (Boston scientific, Natick, USA)를 이용하여 동정맥루에 최대한 근접하여 동정맥루 내에 Gianturco metallic coil(Cook, Bloomington, USA) 3개와 N-butyl-2-cyanoacrylate(Histoacryl, B. Braun, Melsungen, Germany)와 리피오돌 1:3 혼합액 0.5 ml로 색전술을 시행하였다. 색전 후 시행한 골반 혈관조영술상 동정맥루는 더 이상 조영되지 않았으며, 다른 합병증 없이 시술을 종료하였다.
시술 다음날 시행한 color doppler 초음파상 동정맥루의 소실 및 하극 신동맥의 정상적인 분포를 확인하였다.
Fig. 2.
Initial pelvic angiogram (A) shows a renal arteriovenous fistula (arrow) in the lower pole of the transplanted kidney with early draining vein (open arrow) to the vena cava. Selective renal angiogram (B) shows more detailed delineation of the arteriovenous fistula. Final right internal iliac angiogram (C) shows occlusion of the arteriovenous fistula and preservation of the lower lobar artery of the transplanted kidney.
Fig. 3.
Color Doppler US obtained the day after embolization shows non-visualization of the arteriovenous fistula (arrow) in the lower pole of the transplanted kidney
고찰
신장이식 후 다양한 합병증이 발생 할 수 있는데, 이중 혈관 관련 합병증도 1~2% 차지하며, 신동맥 협착, 그로 인한 경색, 동정맥루 및 가성동맥류, 신정맥 혈전 등이 있다. 대부분의 이식신 동정맥루는 이식 거부반응이 의심되어 시행한 생검 이후 발생하고, 육안적 혈뇨가 5~7% 빈도로 발생하나 대부분 자연 치유된다. 본 증례와 같이 자연적으로 지연되어 발생하는 경우는 매우 드물다. 대개 color doppler 초음파를 통해 진단하는데, 동정맥루와 가성동맥류는 정상 혈관 범위에서 이탈한 disorganized color 형태의 국소 병변으로 관찰되고, 특히 동정맥루는 분절동맥(segmental artery) 또는 엽간동맥(interlobar artery)과 분리된 비정상적으로 높은 속도의 와류로 나타난다. Doppler 초음파상 유입동맥은 고속도와 저저항성을 띄고, 유출정맥은 동맥성 파동을 보인다.
생검 이후 발생한 합병증은 대부분 보존적 치료를 통해 호전되어지나, 동반된 가성동맥류의 크기가 증가하거나 크기 2cm 이상으로 큰 경우는 인터벤션 시술을 통한 치료가 필요하며, 미세카테터를 통해 유입동맥을 초선택한 후 색전술을 시행하는 것이 이상적인 치료방법이다. Tarif 등은 자가 혈전, 젤폼, 코일, 탈착형 실리콘 풍선 등 다양한 색전물질을 사용하여, 자가신 생검 후 생긴 동정맥루의 91%와 동종 이식신 생검 후 생긴 동정맥루에 대한 성공적인 색전술 결과를 발표한 바 있다. 그러나 만약 동정맥루가 큰 경우 젤폼과 같은 과립형 색전물질은 동정맥루를 지나 전신순환을 할 수 있기 때문에 동정맥루의 크기, 병변을 일으킨 동맥 단계, 색전물질을 사용하는 시술자의 숙련도에 따라 색전물질 선택에 신중을 기해야 할 것이다.
참고문헌
1. Akbar S, Jafri Z, Amendola M, Madrazo B, Salem R, Bis K. Complications of renal transplantation. RadioGraphics 2005; 25:1335-1356.
2. Vignali C, Lonzi S, Bargellini I, et al. Vascular injuries after percutaneous renal procedures: treatment by transcatheter embolization. Eur Radiol 2004; 14:723-729.
3. Libicher M, Radeleff B, Grenacher L, et al. Interventional therapy of vascular complications following renal transplantation. Clin Transplant 2006; 20:55-59.
Citations
Citations to this article as recorded by