중심단어
Embolization, mesenteric injury, blunt abdominal trauma
임상소견
보행자 TA로 내원하였고 내원 당시 저혈량 쇼크 상태로 BP 60/40mmHg, PR 52회, 환자의 혈색소 수치는 5.7 g/dL로 현저히 감소 되어 있었다
영상소견
조영증강 복부 CT검사에서 우하복부 장간막에 커다란 혈종과 출혈이 관찰 되었다(Fig. 1). 장손상을 시사할 만한 소견이나 다른 복부 장기에 동반된 손상은 없었다. 좌측 골반의 장골 골절이 관찰되었지만 급성출혈은 동반하지 않았다. 뇌 CT검사에서는 외상에 의한 지주막하출혈 소견이 관찰되었다. 일차적으로 수술적 치료를 고려하였으나, 환자의 전신상태의 악화로 인한 위험성 및 개복술의 과거력에 의한 장간막 유착의 가능성, 복강내 다른 장기의 동반 손상이 없었기 때문에 외과의는 응급 개복술 대신 동맥색전술을 의뢰하였다.
시술방법 및 재료
수혈과 동시에 5F RH catheter(Cook, Bloomington, USA)를 이용하여 상장간막동맥조영술을 시행하였고, right ileal artery 및 ileocolic artery에서 가성동맥류들과 복강 내로의 조영제 유출들이 관찰되었다(Fig. 2). 2.9F coaxial microcatheter(Stride, ASAHI, Aichi, Japan)를 이용하여 가성동맥류의 원위부까지 위치시키려 하였지만 쇼크에 의한 혈관수축으로 진행시키지 못하고 근위부에서 gelatin sponge(Cutanplast, Mascia Brunelli, Milan, Italy)를 이용하여 색전술을 시행하였다(Fig. 3A, B). 색전된 동맥에서 공급되는 장에 측부혈류를 통한 혈관공급이 관찰되었다(Fig. 3C). 수혈과 색전술 후 환자의 혈압은 123/72mmHg로 증가하였다. 환자의 전신상태가 호전된 후 장간막의 혈종의 제거 및 장간막 손상을 치료하기 위해 개복술을 시행하였다. 육안적 수술소견에서는 대장 및 소장벽에 경색 혹은 허혈을 시사할 만한 소견은 없었다.
고찰
Blunt abdominal trauma(BAT)에 있어서 장간막의 손상은 비교적 드물지만 사망률과 이환율의 결정에 매우 중요한 요인을 제공한다. BAT에 의한 혈역학적으로 불안정한 환자에서 CT영상에 의한 조기진단 및 응급개복술이 가장 표준화된 방법이지만, 이러한 수술적 치료에도 불구하고 장간막 손상에 의한 사망률 및 이환율은 지속적으로 높게 나타나며, 복부 이외의 다른 장기 특히 두부손상이 동반된 경우는 더욱 증가한다(1). 장간막 손상의 치료는 CT검사에서 장간막 혈종과 함께 장벽에 직접적인 손상을 암시하는 장벽의 불연속성이나 장외공기 등이 보이는 경우나, 혈류저하 등이 의심되는 장벽 비후나 조영증강 등이 보일 경우 수술적 치료를 선택한다(2).
그러나 점차 비수술적 치료방법의 발달로 수술을 대체 할 수 있는 일차적 치료 방법으로 TAE(transcatheter arterial embolization)를 선택 하는 경우들이 있다. 환자의 상태가 수술적 조건에 적합하지 않거나, 수술에 앞서 전처치로 일과성의 치료가 요구되는 경우들에 있어서 TAE는 효과적이다(3, 4). 특히 장벽손상의 증거가 뚜렷하지 않고, 독립된 장간막 손상만 있는 경우 TAE를 고려 할 수 있으며, 수술적 치료 없이 TAE만으로도 치료된 경험들을 보고하고 있다(5-7). 혈관의 색전술을 시행하기 전·후에 목표혈관의 원위부에 있는 측부혈류를 확인하는 것이 중요하며, 측부혈류가 있는 경우는 색전술 후 장경색의 가능성이 줄어든다. 대부분은 marginal artery를 통하여 측부혈류가 형성되어 원위부의 vasa recta까지 혈류가 잘 유지 되므로, 대부분의 문헌들에서는 색전술 후 장허혈 등의 합병증 없이 치료가 잘 되었던 경우들을 보고하고 있다(5, 6, 8). 가성동맥류의 경우는 근위부와 원위부를 색전하는 것이 중요하지만, 다른 보고들 및 우리의 경험과 마찬가지로 혈관의 파열 및 수축으로 microcatheter를 원위부까지 삽입이 불가능한 경우가 많기 때문에, 근위부의 색전술만으로 측부혈류에 의한 출혈이나 가성 동맥류의 재발 없이 효과적인 치료를 할 수 있었다.
이번 증례에서도 장간막에 급성출혈 및 혈역학적인 불안정이 있었기 때문에 수술적 치료를 요하였으나, 다른 복부 장기에 동반손상 없이 국소성 장간막 손상, 개복술의 과거력에 따른 유착의 가능성, 환자상태의 심각한 악화 및 동반된 뇌손상에 따른 사망률 및 이환율의 증가, 수술의 위험성 등을 고려하여 TAE를 우선 시행하였고, 환자상태의 회복 후 수술적 치료를 계획하였다. 외상에 의한 장간막 출혈은 드물지만 임상적으로 환자의 예후에 매우 중요한 임상소견이다. 대부분은 일차적 치료방법으로 수술을 선택하지만, 장손상이나 허혈 및 복강내 다른 동반된 장기의 손상이 없는 경우 TAE는 수술을 대체, 보조할 수 있는 유용한 방법이다.
참고문헌
1. Davis JJ, Cohn JR, Nance FC. Diagnosis and management of blunt abdominal trauma. Ann Surg 1976; 183:672-678.
2. Dowe MF, Shanmuganathan K, Mirvis SE, Steiner RC, Cooper C. CT findings of mesenteric injury after blunt trauma: implications for surgical intervention. AJR 1997; 168:425-428.
3. Gabata T, Matsui O, Nakamura Y, Kimura M, Tsuchiyama T, Takashima T. Trancatheter embolization of traumatic mesenteric hemorrhage. JVIR 1994; 5:891-894.
4. Rundback JH, Chughtai S, Rozenblit G, et al. Traumatic ileocolic pseudoaneurysm: diagnosis and transcatheter treatment. Cathet Cadiovasc Intervent 1999; 48:217-219.
5. Kakizawa H, Toyota N, Hieda M, et al. Traumatic mesenteric bleeding managed solely with transcatheter embolization. Radiat Med 2007; 25:295-298.
6. Kondo N, Sakashita Y, Sugihara M, et al. Ruptured left colic arterial aneurysm treated by transcatheter arterial embolization alone and without a subsequent laparotomy: report of a case. Surg Today 2011; 41:707-712.
7. Asayama Y, Matsumoto S, Takuro I, et al. A case of traumatic mesenteric bleeding controlled by only transcatheter arterial embolization. Cardiovasc Intervent Radiol 2005; 28:256-258.
8. Hagiwara A, Takasu A. Transcatheter arterial embolization is effective for mesenteric hemorrhage in trauma. Emer Radiol 2009; 16: 403-406.
Fig. 1.
Fig. 1. Contrast enhanced CT demonstrates mesenteric hematoma with some areas of contrast extravasation(arrows), indicating active bleeding. Also, the fracture of the left pelvic bone is noted.
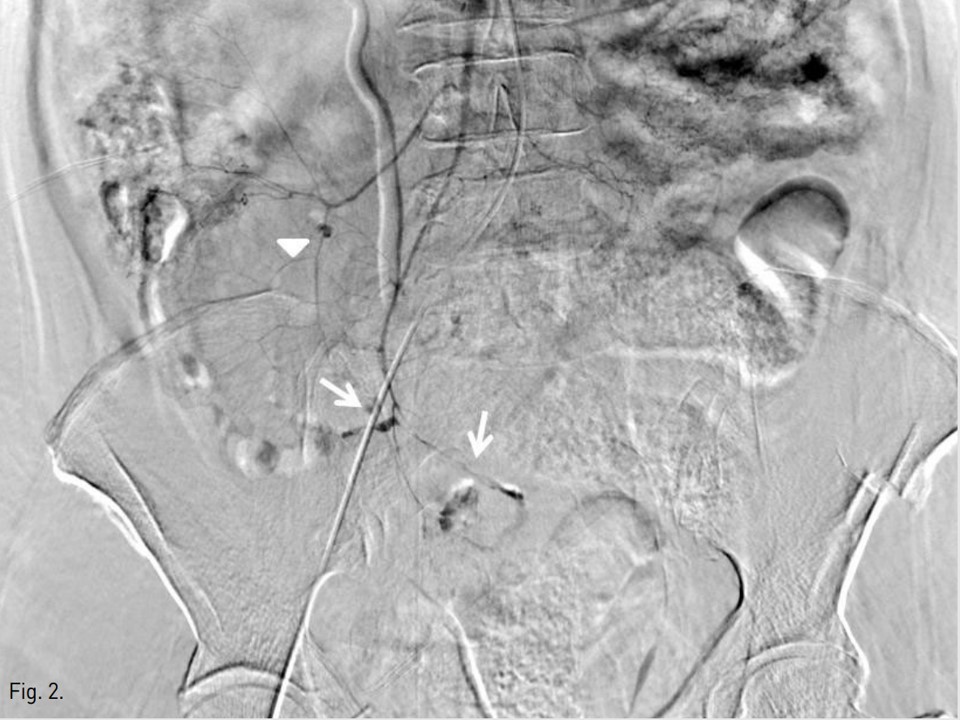
Fig. 2.
Fig. 2. Superior mesenteric angiogram demonstrates multiple pseudoaneurysms with extravasation of contrast media at distal branches of ileocolic (arrows) and right colic (arrowhead) arteries.
Fig. 3. A
Fig. 3A, B. Ileocolic (A) and right colic (B) arterial branches were embolized by using gelatin sponge, respectively(arrows).
Fig. 3. B
Fig. 3A, B. Ileocolic (A) and right colic (B) arterial branches were embolized by using gelatin sponge, respectively(arrows).
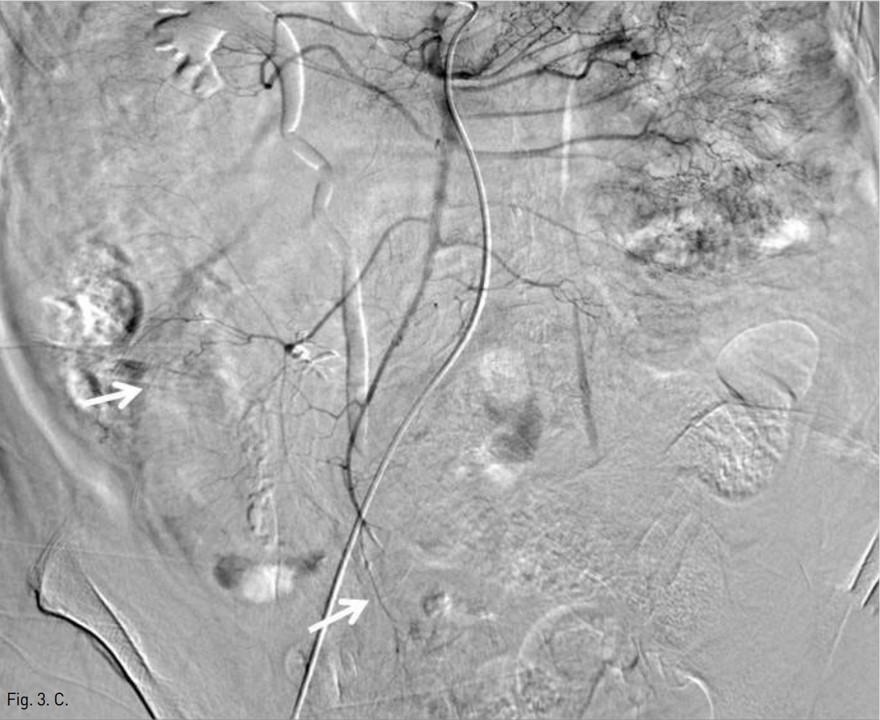
Fig. 3. C
Fig. 3C. Superior mesenteric angiogram after TAE demonstrates occlusion of the pseudoaneurysms with preserving blood supply to the affected bowels (arrows).
Citations
Citations to this article as recorded by