중심단어
Bronchial artery embolization, Hemoptysis, CT angiography
임상소견
30년 전 폐결핵 치료를 받은 환자로 최근 2개월 동안 2 차례 객혈하여 치료 위해 입원하였음.
진단명
Hemoptysis associated with pulmonary tuberculosis
영상소견
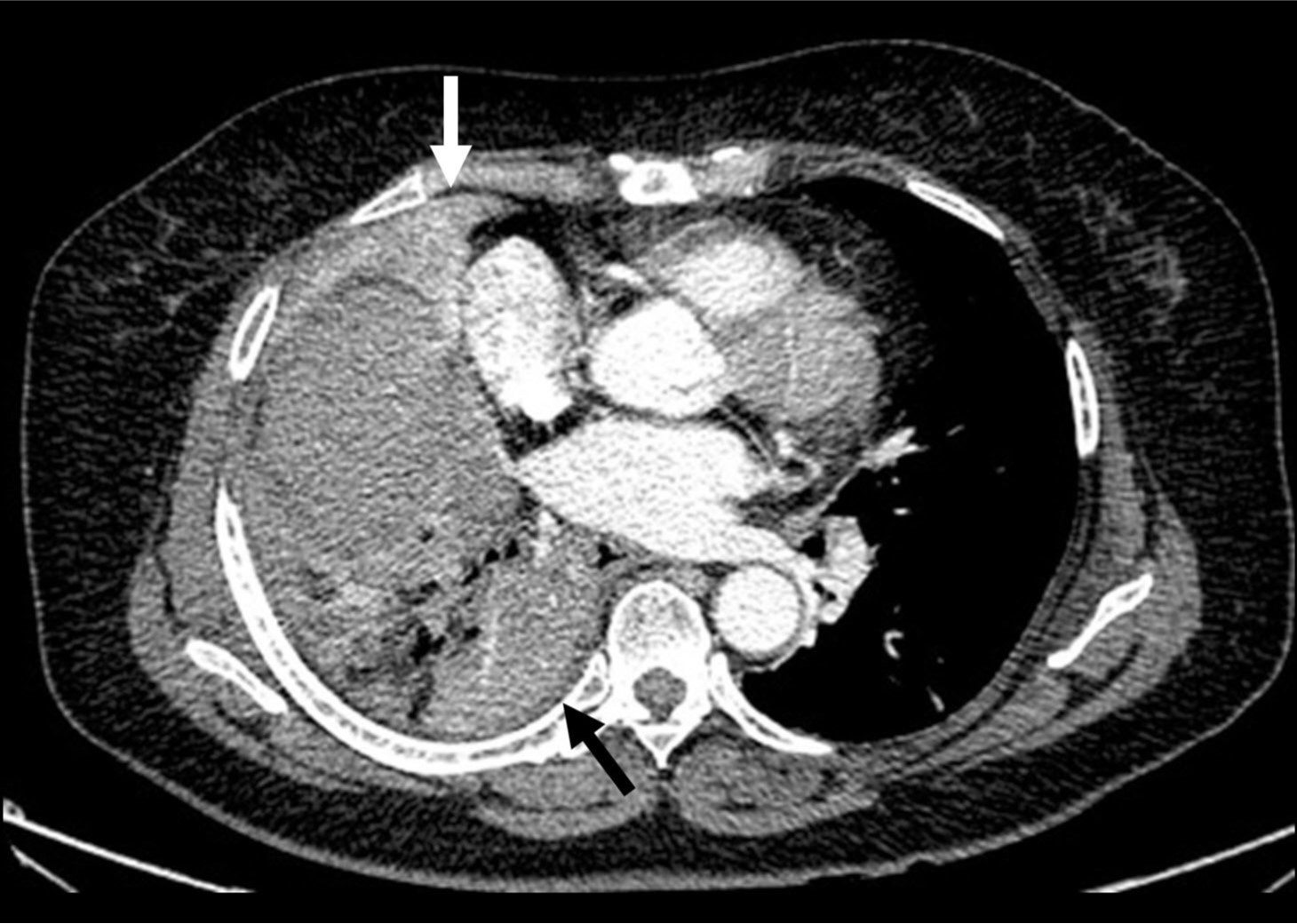
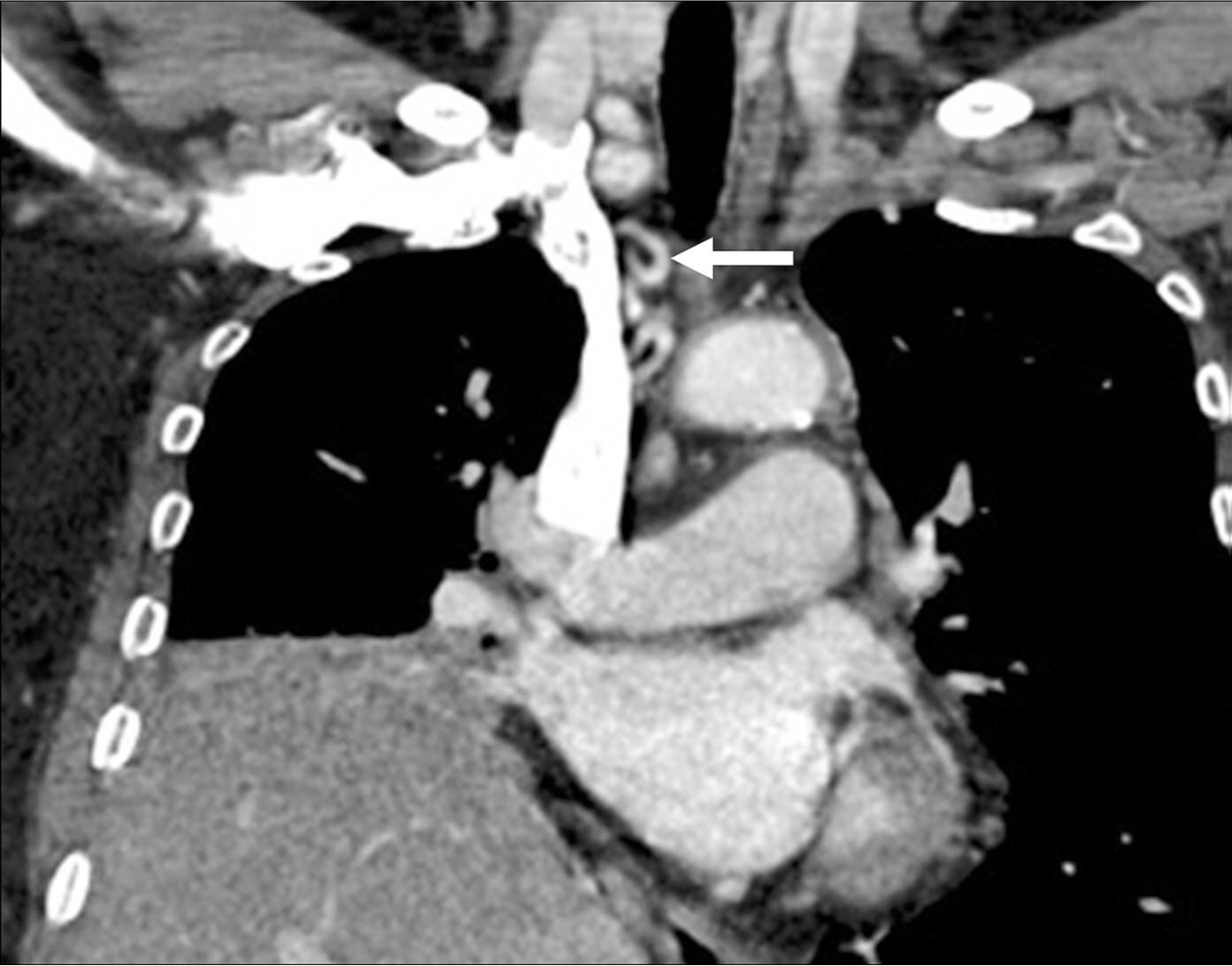
흉부 CT영상에서 우측 폐 중엽 및 하엽 기관지 내경 감소 및 anthracofibrosis가 의심되었고, 원위부 우중엽과 우하엽에 폐쇄성 무기폐 소견이 관찰되었으며 우기관지동맥이 우쇄골하동맥 근위부에서 기원하는 것으로 추정되었음(Fig. 1). 기관지내시경에서 우중엽에서 출혈이 관찰되었음.
시술방법 및 재료
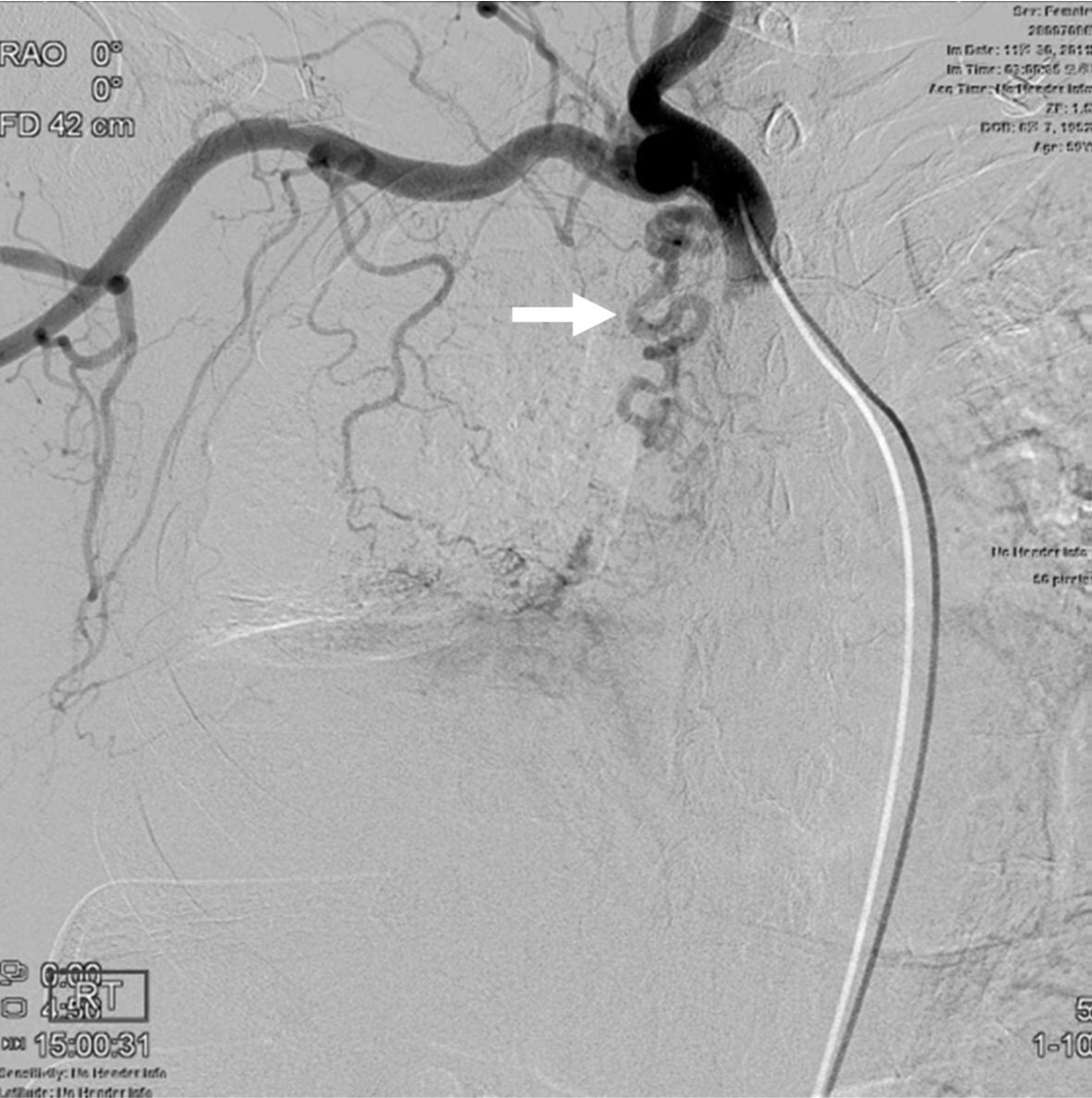
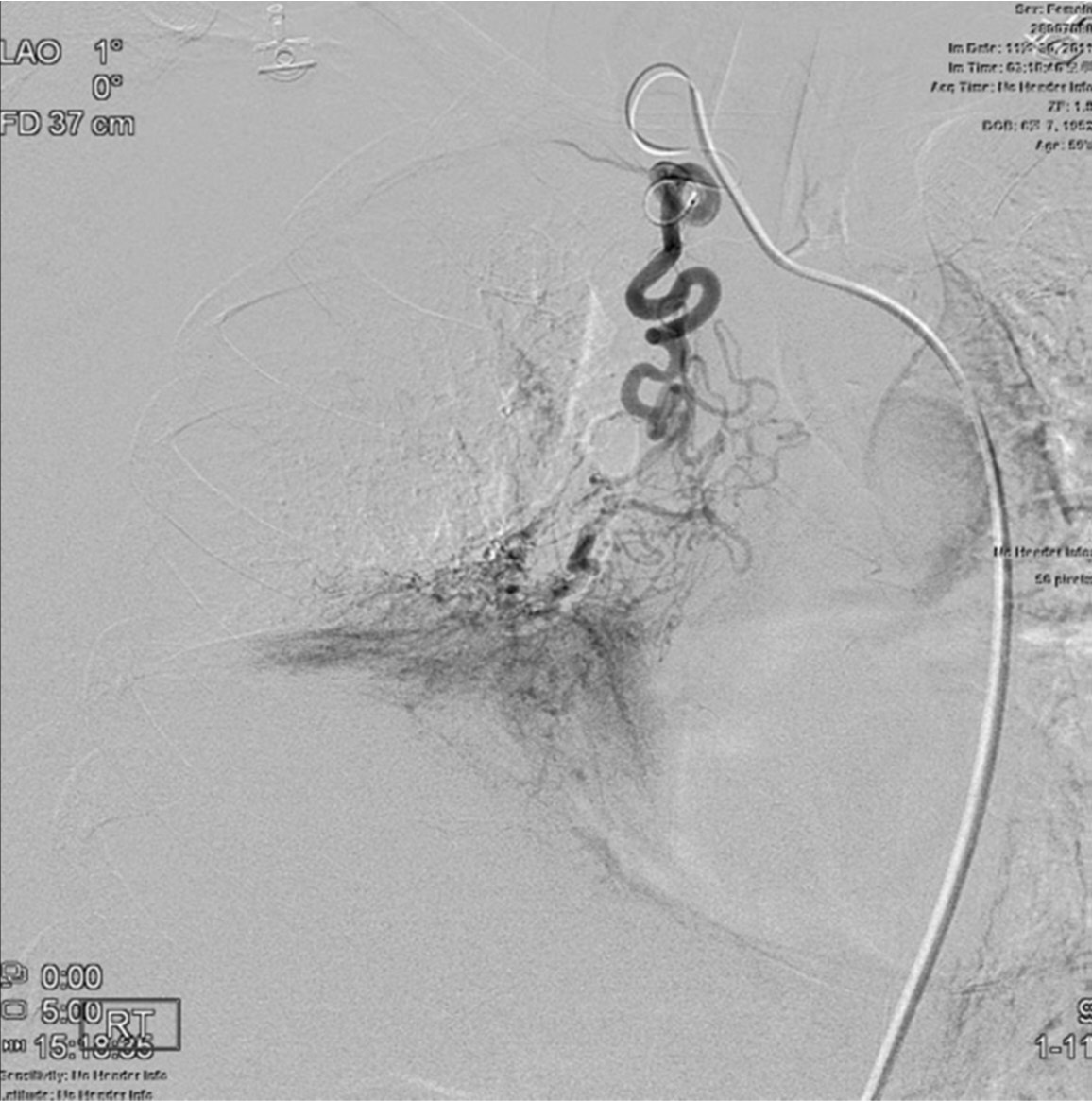
우대퇴동맥을 천자한 후 5F 카테타를 흉부대동맥까지 전진하여 시행한 흉부대동맥조영술에서 굵어진 우늑간동맥들과 우횡경막하동맥이 관찰되었지만 우기관지동맥은 안보였다(Fig. 2). CT영상에서 우기관지동맥이 우쇄골하동맥에서 기시하는 것으로 추정되어 5F 카테타로 우쇄골하동맥조영술을 시행하였고 굵어진 우기관지동맥이 우쇄골하동맥 근위부에서 기시하는 것을 확인하였다(Fig. 3A). 2.2F 미세도관(Progreat, Terumo, Tokyo, Japan)으로 선택적 우기관지동맥조영술을 시행하여 객혈의 원인이 될 수 있는 우하폐야 실질의 과혈관성을 확인한 후(Fig. 3B) 500 - 700um PVA입자(Boston Scientific, Natick, USA)로 우기관지동맥을 색전하였다. 굵어진 우늑간동맥들의 선택적 혈관조영술을 시행하였을 때 우하폐야 과혈관성 등의 이상소견은 안보였고, 우신동맥에서 기시하는 우횡경막하동맥의 선택적 혈관조영술을 시행하였을 때 굵어진 동맥에 의한 우하폐야 실질의 과혈관성 및 폐순환단락이 관찰되었다(Fig. 4). 우횡경막하동맥도 2.2F 미세도관으로 초선택한 후 500 - 700um PVA입자로 색전하였다. 색전술 후 동맥조영술에서 우기관지동맥과 우횡경막하동맥의 혈류는 거의 차단되었고 우하폐야의 과혈관성 및 폐순환 단락은 소실되었다.
고찰
기관지동맥 색전술은 대량 객혈의 치료로서 최소침습적이면서도 가장 효과적인 치료법으로 알려져 있다. 시술 후 즉시 객혈의 증상이 조절되는 빈도는 73-99%로 보고되고 있다. 그러나 기관지동맥 색전술 후 1달 내 객혈의 재발율은 10-29%로 비교적 높다고 알려져 있으며 장기적으로도 색전된 혈관의 재개통이나 곁순환의 형성 등으로 재발의 가능성이 있다.
기관지동맥은 해부학적 변이가 흔하여 기시부의 위치 및 분지하는 형태가 다양하다. 가장 흔한 기시부의 위치는 5번 흉추 상부 경계와 6번 흉추 하부 경계 사이 흉부대동맥이며(70%-83.3%), 이외에 대동맥궁, 상완두동맥간, 쇄골하동맥, 내흉동맥, thyrocervical trunk, costocervical trunk, 복부대동맥, 횡경막하동맥, 관상동맥 등에서 기시할 수 있다. 기관지동맥이 분지하는 형태는 intercostobronchial trunk(88.7%)의 형태가 가장 흔하지만 기관지동맥이 독립적으로 기시하는 경우도 빈번하며 좌우측 기관지 동맥의 개수는 하나에서 여러 개가 존재할 수 있다.
한편 대량 객혈의 원인이 되는 혈관이 기관지동맥이 아닌 non-bronchial systemic artery인 경우도 있으며 그 빈도는 41-88%로 다양하게 보고되고 있다. 이 경우 늑간, 쇄골하, 액와, 내흉, 횡경막하동맥 등의 다양한 체순환계 혈관들이 원인이 된다고 알려져 있다. 따라서 대량 객혈을 호소하는 환자의 성공적인 기관지동맥 색전술을 위해서는 시술 전 동맥기 CT영상을 필수적으로 얻어야 한다. 동맥기 CT영상에서 기관지동맥의 해부학적 특성 및 non-bronchial systemic artery에서의 객혈 가능성 여부를 시술자가 사전에 파악할 수 있기 때문에, 기관지동맥 색전술을 효과적, 효율적으로 시행할 수 있게 된다. 본 증례에서도 우기관지동맥이 우쇄골하동맥에서 기시하는 점을 사전 CT영상에서 인지함으로써 기관지동맥 색전술을 효율적으로 시행할 수 있었다.
참고문헌
1. Chun J, Morgan R, Belli A. Radiological management of hemoptysis: A comprehensive review of diagnostic imaging and bronchial arterial embolization. Cardiovasc Intervent Radiol 2010; 33:240-250.
2. Noe GD, Jaffe SM, Molan MP. CT and CT angiography in massive haemoptysis with emphasis on pre-embolization assessment. Clinical Radiology 2011; 66:869-875.
3. Yoon W, Kim YH, Kim JK, Park JG, Kang HK. Massive hemoptysis : prediction of nonbronchial systemic arterial supply with Chest CT. Radiology 2003; 227:232-238.
Fig. 1. A
Fig. 1A. Chest CT scan shows atelectasis of right middle and lower lobes (arrows).
Fig. 1. B
Fig. 1B. A tortuous and dilated artery (arrow), suspected to be the right bronchial artery, appears to be originated from the right subclavian artery.
Fig. 2.
Fig. 2. Thoracic aortogram shows no demonstration of the right bronchial artery and hypertrophy of the right inferior phrenic (arrowheads) and intercostal (arrows) arteries.
Fig. 3. A
Fig. 3A. Right subclavian arteriogram reveals hypertrophy of the right bronchial artery (arrow), originated from the proximal part of the right subclavian artery.
Fig. 3. B
Fig. 3B. Hypervascular parenchymal staining in the right lower lung field is demonstrated on selective angiogram of the right bronchial artery.
Fig. 4.
Fig. 4. Selective angiogram of the right inferior phrenic artery shows arterial hypertrophy, hypervascular parenchymal staining in the right lower lung field, and shunting to pulmonary circulation (arrow).
Citations
Citations to this article as recorded by