중심단어
Liver injury, blunt trauma, angioembolization
임상소견
당일 발생한 복부 외상에 의한 통증으로 응급실로 내원하였다. 내원 당시 활력 징후는 혈압 120/80mmHg, 맥박수 99/min였고, 혈색소 수치는 8.6g/dL였다.
진단명
Liver injury with a large subcapsular hematoma after trauma
영상소견
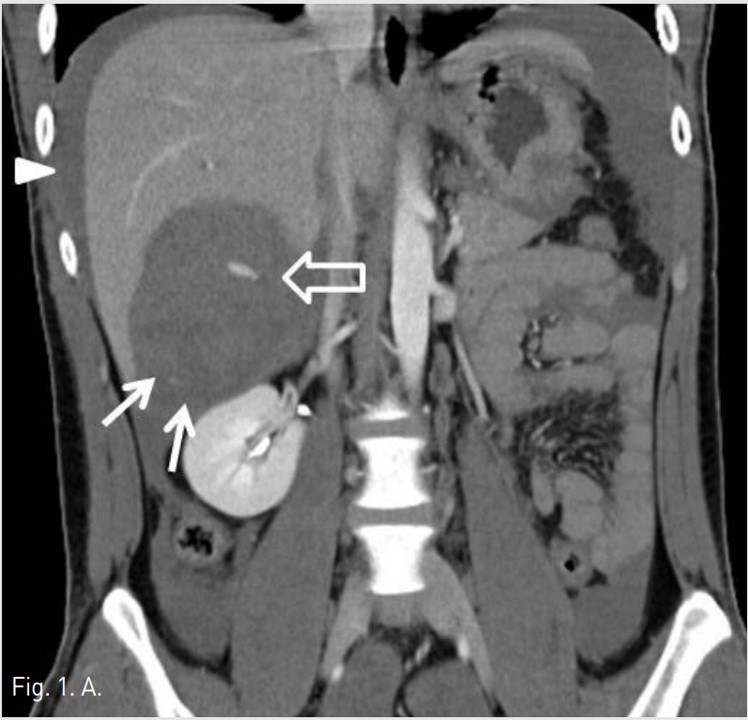
응급실에서 시행한 복부 CT검사에서 복강내 출혈 및 간 우엽의 후면을 따라 국소성 피막하혈종이 보였고, 내부에 출혈을 시사하는 조영제 유출이 보였다(AAST[American Association for the Surgery of Trauma] gradeⅡ)(Fig. 1A).
시술방법 및 재료
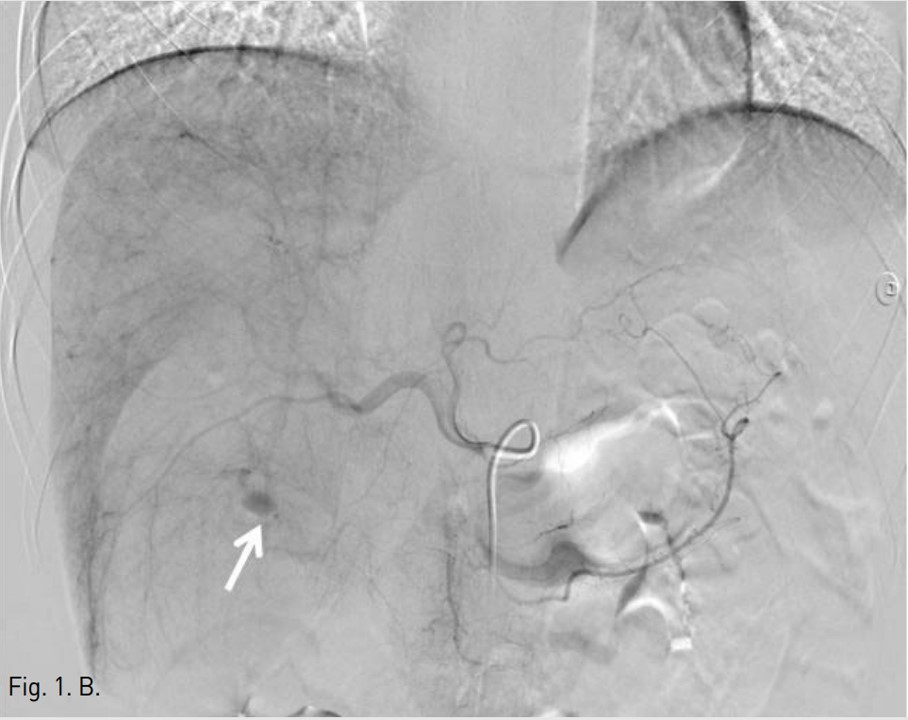
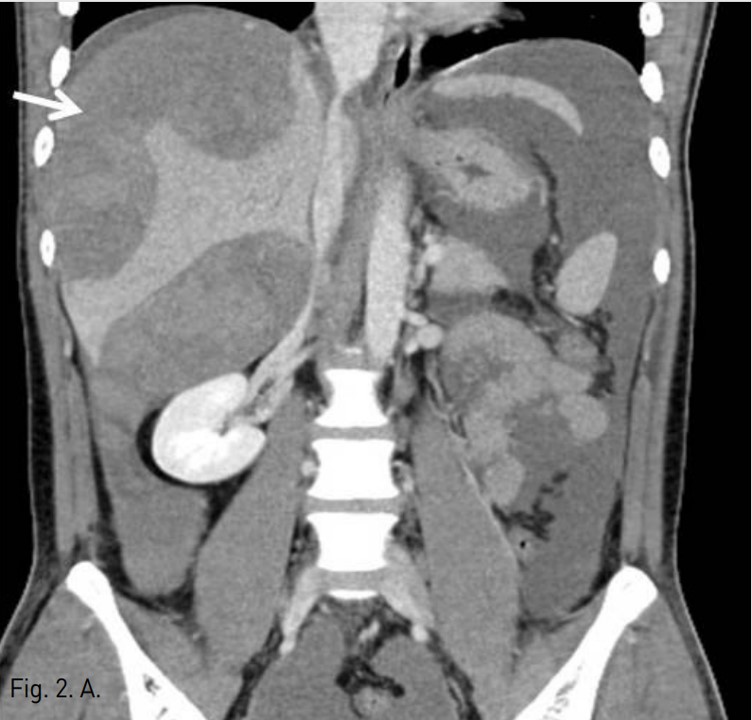
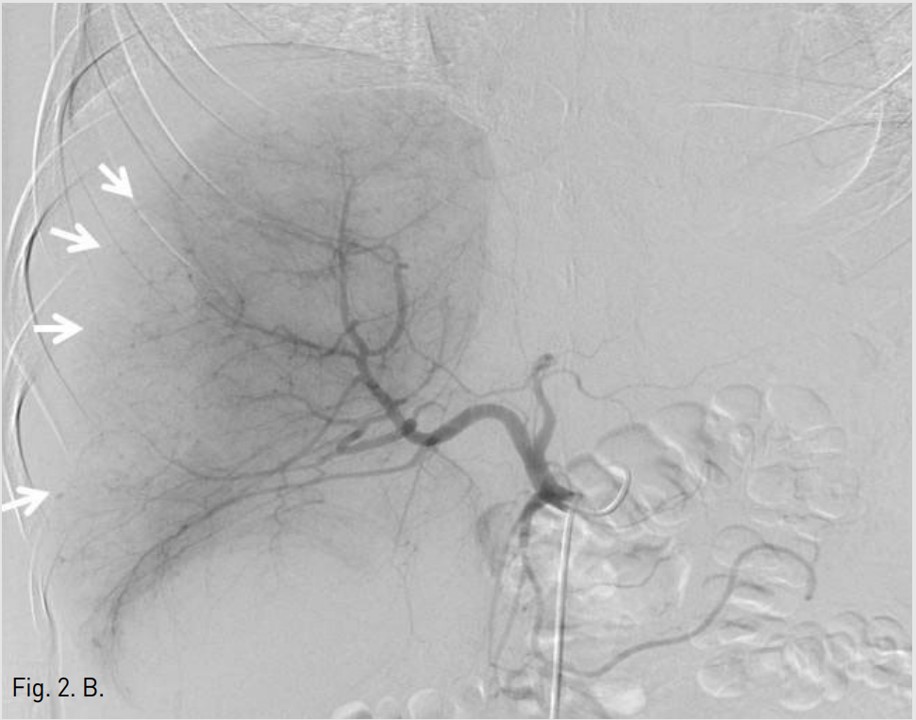
5F RH catheter (Cook, Bloomington, USA)를 이용하여 바로 시행한 간동맥조영술에서 right posterior inferior hepatic branch에서 급성출혈이 관찰되었다(Fig. 1B). 2.9F coaxial microcatheter(Stride, ASAHI, Aichi, Japan) 로 출혈혈관부위를 초선택한 후 gelatin sponge(Cutanplast, Mascia Brunelli , Milan, Italy)을 이용하여 색전술을 시행하였다(Fig. 1C). 시술 다음날 혈색소 수치는 10.0g/dL로 증가하였다. 그러나 시술 2일 후 환자의 활력징후는 혈압 131/80mmHg, 맥박수 82/min로 안정적이었지만, 혈색소가 7.8g/dL로 급격히 감소하였고, 우상복부에 심한 통증을 호소하여 재출혈의 의심하에 복부 CT검사를 시행하였다. CT검사에서 간에 다량의 피막하 혈종이 관찰되었지만, 조영제의 혈관외 유출은 보이지 않았다(AAST grade Ⅲ)(Fig. 2A). 같은 날 시행한 간동맥 혈관조영술에서 기존 색전술을 시행한 동맥에서의 재관류는 없었지만, 새로 생긴 다른 부위의 피막하혈종 내로 광범위한 다발성 미세출혈이 관찰되었다(Fig. 2B). Microcatheter를 이용하여 각 출혈부위 근처의 segmental artery들을 선택한 후 gelatin sponge를 이용하여 광범위한 부위에 색전술을 시행하였고, 더 이상의 출혈은 관찰되지 않았다(Fig. 2C, D). 시술 후 환자의 혈색소는 정상화되었고 우상복부 통증은 점차 감소하였다. 이 후 뚜렷한 합병증 없이 입원 1달 후 퇴원하였다.
고찰
외상에 의한 간손상의 경우 치료방법의 결정은 환자의 혈역학적인 안정성, 중증환자의 집중치료 가능여부, 응급수술을 수행할 수 있는 능력 등 다양한 요인들을 고려하여 결정한다. 혈역학적으로 안정한 환자의 대부분은 TAE(trans catheter arterial embolization)를 포함한 비수술적 치료방법을 선택한다(1-3). 그러나 비수술적 치료에 의해 지연출혈, 농양, 가성동맥류, hemobilia, biloma, bile peritonitis 등의 다양한 합병증들이 발병할 수 있으며, 다양한 중재적 시술을 통하여 대부분 치료가 가능하다. 비수술적 치료에 의해 발생되는 합병증의 빈도는 5-23%이고, 이 중 지연성 출혈은 가장 흔한 합병증이며 약 18%의 사망률을 보인다(4). 지연성 출혈은 최초의 경미한 손상이 확대되었거나, biloma에 의한 가성동맥류의 형성에 의한다(5). 지연 혹은 이차 출혈의 빈도는 0-14%까지 보고 되고 있고, 외상에서부터 파열까지의 경과시간은 8시간부터 30일까지 다양하며 대부분 72시간 이내에 발생한다(5, 6). 임상양상은 지속적인 수혈의 필요, 혈색소 수치의 저하, 상복부의 지속적 통증 등이 있는 경우 지연성 출혈을 의심하여야 하며, 영상검사에서 간내 출혈 혹은 피막하혈종의 증가를 확인할 수 있다. 지연성 간출혈의 치료는 환자의 혈역학적 상태에 따라 혈관색전술이나 수술적 치료를 고려해야 하며, 대부분 혈역학적으로 안정적인 경우 경도관 동맥색전술을 시행하며, 불안정한 경우에는 수술적 치료를 요하지만, 여러 문헌들에서 경도관 동맥색전술을 성공적으로 시행한 경험들을 보고하고 있다(6-8). 또한 AAST grade Ⅳ 이상의 심한 간손상 환자에 있어서도 TAE를 성공적으로 시행 할 수 있다(2). 본 증례는 외상 2일 후 지연성 출혈에 의해 간에 광범위한 다량의 피막하 혈종이 관찰되었던 경우로, CT에서 급성출혈은 보이지 않았지만, 간동맥조영술에서 간의 우엽의 대부분의 말단동맥들에서 미세한 출혈들을 확인할 수 있었다. 경도관 동맥색전술로 간의 우엽 2/3 정도의 segmental artery들을 색전하였지만 간기능 저하를 포함한 다른 합병증 없이 지연성 출혈을 치료할 수 있었다.
지연성 간출혈에 있어서 치료는 비수술적 치료 대신 수술적 치료의 선택을 선호하는 주장도 있지만(9), 문헌에 보고된 사망률의 대부분은 수술을 시행한 군에서 집계 되었다(4). TAE는 대량의 지연성 간출혈의 경우에도 수술을 대체 할 수 있는 효과적인 치료 방법으로 사용될 수 있다.
참고문헌
1. Ahmed N, Vernick J. Management of liver trauma in adults. J Emerg Trauma Shock 2011; 1:114-119.
2. Monnin V, Sengel C, Thony F, et al. Place of arterial embolization in severe blunt hepatic trauma: a multidisciplinary approach. Cardiovasc Intervent Radiol 2008; 31:875-882.
3. Gourgiotis S, Vougas V, Germanos S, et al. Operative and nonoperative management of blunt hepatic trauma in adults: a single-center report. J hepatobiliary Pancreat Surg 2007; 14:387-391.
4. Fisher JC, Moulton SL. Nonoperative management and delayed hemorrhage after pediatric liver injury: new issues to consider. J Pediatr Surg 2004; 39619-622.
5. Goffete PP, Laterre PF. Trasumatic injuries: imaging and intervention in post-traumatic complications (delayed intervention). Eur Radiol 2002; 12:994-1021.
6. Hagiwara A, Yukioka T, Shimazaki S, et al. Delayed hemorrhage following transarterial embolization for blunt hepatic injury. Cardiovasc Intervent Radiol 1993; 16:380-383.
7. Giss SR, Dobrilovic N, Brown RL, Garcia VF. Complications of nonoperative management of pediatric blunt hepatic injury: diagnosis, management, and outcomes. J Trauma 2006; 61:334-339.
8. Kozar RA, Moore JB, Niles SE, et al. Complications of nonoperative management of high-grade blunt hepatic injuries. J Trauma 2005; 59:1066-1071.
9. Sjovall A, Hirsch K. Blunt abdominal trauma in children: risk of nonoperative treatment. J Pediatr Surg 1997; 32:1169-1174.
Fig. 1. A
Fig. 1A. Initial coronal CT scan shows a large subcapsular hematoma (arrows) with extravasation of contrast media (open arrow) inferior to the right hepatic lobe and perihepatic fluid collection, indicating hemoperitoneum (arrowheads).
Fig. 1. B
Fig. 1B. Celiac angiogram shows active bleeding (arrow) from a branch of the right hepatic artery. After selective catheterization of the bleeding artery with a 2.9 F microcatheter, the artery was embolized by using gelatin sponge.
Fig. 2. A
Fig. 2A. The coronal CT image obtained 2 days after embolization shows a large diffuse expanding subcapsular hematoma (arrow).
Fig. 2. B
Fig. 2B. Celiac angiogram during second embolization shows multiple tiny contrast extravasations in right subcapsular area (arrows).
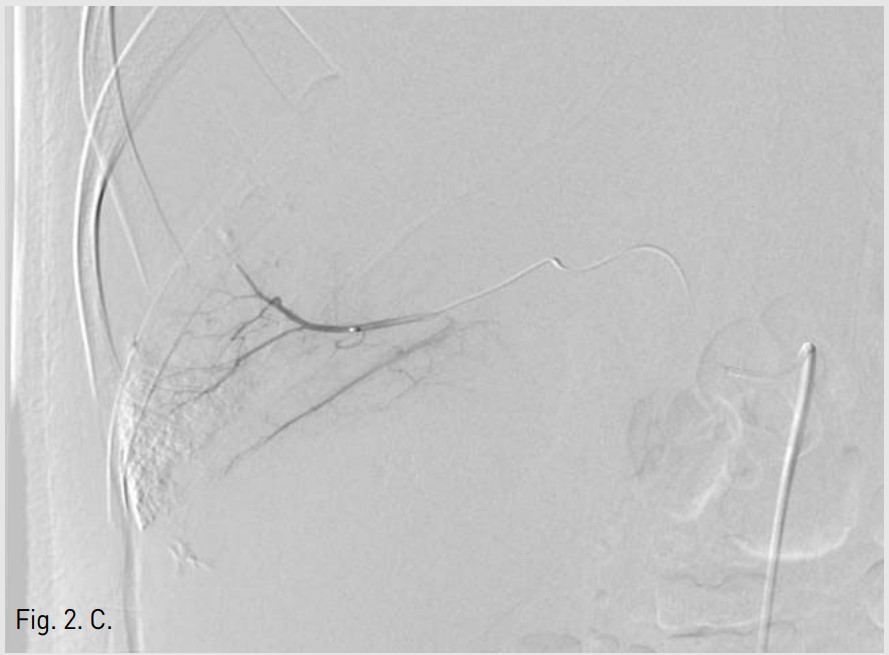
Fig. 2. C
Fig. 2C. After selective catheterization of multiple bleeding arteries with a microcatheter, embolization was performed by using gelatin sponge.
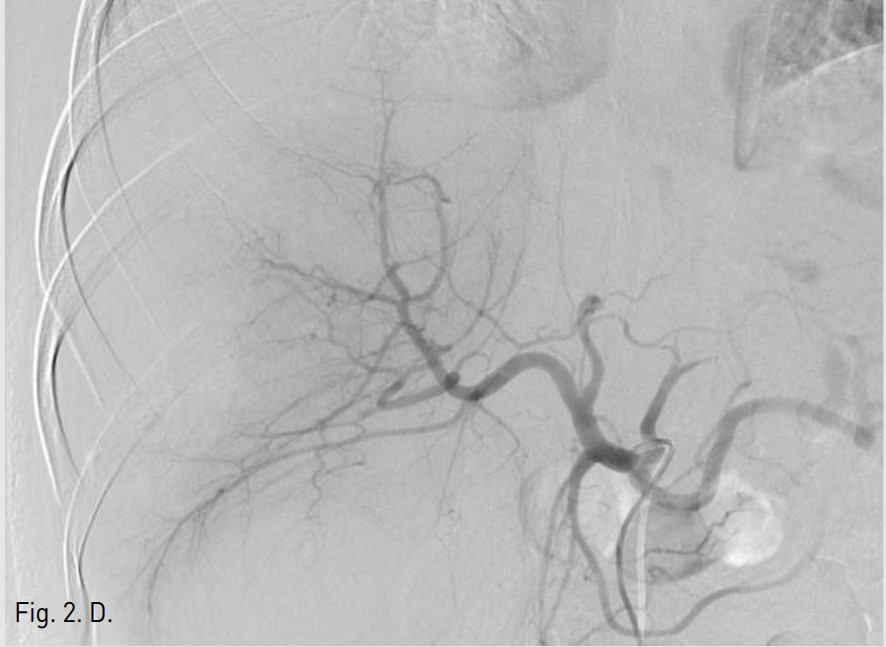
Fig. 2. D
Fig. 2D. Post-embolization angiogram shows no evidence of arterial bleeding.
Citations
Citations to this article as recorded by