중심단어
Aberrant ovarian collateral artery, external iliac artery, uterine artery embolization
임상소견
4년전과 7년전에 자궁근종 절제술을 시행 받았던 과거력이 있는 35세 여자 환자가 6개월간의 월경과다를 주소로 내원하였다.
영상소견
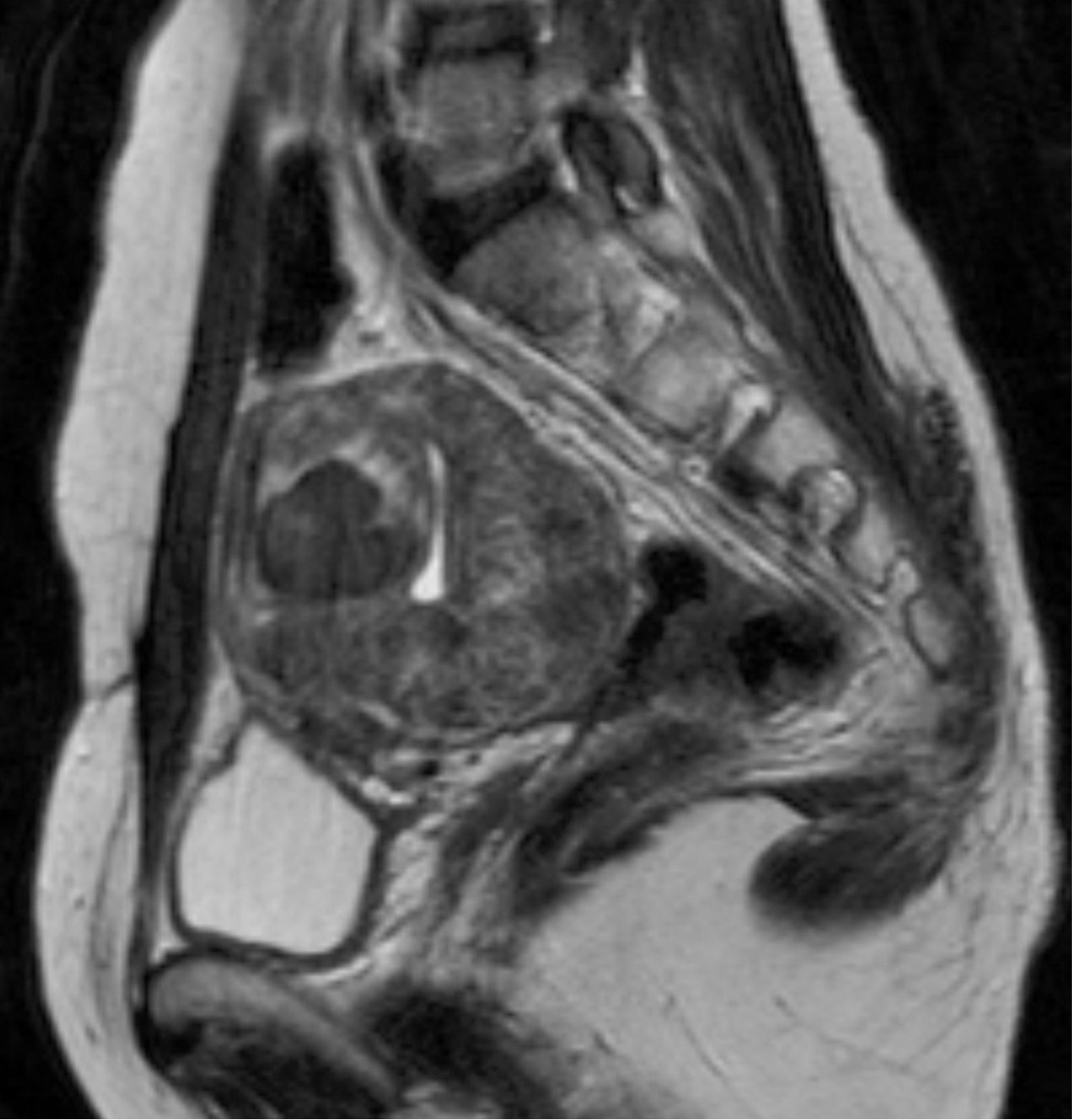
자기공명영상에서 조영증강이 되는 다발성 자궁근종이 있었고, 가장 큰 것의 크기는 6.1 x 4.2 x 5.9cm로 측정되었다(Fig. 1).
시술방법 및 재료
초음파 유도 하에 우측 대퇴동맥을 천자하여 5F sheath(Terumo, Tokyo, Japan)를 삽입하였다. Pigtail 카테타(Cook, Bloomington, USA)를 복부 대동맥에 위치시킨 후 골반동맥조영술을 시행한 결과, 좌측 자궁동맥은 커져 있었으나, 우측 자궁동맥은 위축되어 있었다(Fig. 2A). 동시에 우측 바깥엉덩동맥으로부터 기시하는 비대해진 우측 변이 난소측부동맥이 보였다(Fig. 2A). 5F RUC 카테타(Cook, Bloomington, USA)를 우측 외장골동맥에 진입시키고 Microferret 카테타(Cook, Bloomington, USA)로 우측 변이 난소측부동맥을 선택하였다. 난소동맥조영술상에서 우측자궁동맥은 변이 난소측부동맥에 의하여 완전히 대치되어 있었다(Fig. 2C). 양측 자궁동맥 색전술을 시행한 뒤, 추가로 355-500um 크기의 polyvinyl alcohol 색전입자(Contour, Boston Scientific, Natick, USA)를 사용하여 우측 변이 난소측부동맥 색전술을 시행하였고, 10번의 심장박동 동안 동맥 내에 조영제의 정체가 보일 때까지 색전술을 시행하였다. 색전술 후 3개월째 시행한 자기공명영상에서 대부분의 자궁근종들은 완전히 괴사되었으며, 가장 큰 것은 84.4%의 부피감소를 보였다(Fig. 3). 시술 전 증상을 10점으로 가정 하였을 때, 색전술 후 1년째 되는 시점에 생리과다의 증상 점수는 4점으로 감소하였다.
고찰
자궁동맥 색전술은 증상이 있는 자궁근종의 치료에 있어 매우 유용하나(1), 약 4-19%의 경우 성공적인 자궁동맥 색전술 후에도 임상 증상이 지속된다고 한다(2). 이러한 현상의 가장 흔한 원인은 난소측부동맥 순환이 있는 경우로, 5 - 6%의 발생률을 보인다(1, 3). 하지만, 난소동맥 색전술은 난소 기능의 변화와 관련이 있기 때문에, 자궁근종의 위치, 환자의 나이, 임상적 이득, 난소 기능 상실의 위험도 등의 다양한 요소를 고려하여 시행하여야 한다. 일반적으로 난소동맥은 신장동맥 기시부의 아래쪽 대동맥에서 직접 기시하는데, 6-12%에서 신장동맥으로부터 기시한다고 알려져 있다(4, 5). 또한, 부신장동맥이 있을 때, 대동맥보다 부신장동맥에서 난소동맥이 기시하는 경우가 더 많다. Ravery 등에 따르면, 태아기 때 신장이 위로 이동하는 동안, 난소는 위, 아래 신장줄기동맥으로부터 혈류를 공급받게 되는데, 나중에 이 줄기들이 정상적으로 퇴화하지 않으면 변이 난소동맥이 신장동맥으로부터 기원한다고 하였다(6). 인간태아 연구에 따르면, 생식선동맥의 변이는 여자보다 남자, 그리고 좌측보다 우측에서 더 빈번하게 발생한다(7). 드물게 난소동맥이 요추동맥 혹은 총장골동맥으로부터 기시하는 경우도 보고 되었다(8). 본 증례의 경우 외장골동맥에서 기시하는 변이 난소동맥이 있었고, 이 동맥이 우측 자궁동맥을 완전히 대치하고 있을 뿐만 아니라 우측 난소의 혈류공급도 또한 담당하고 있었다. 하복벽동맥으로부터 기시하는 원인대동맥은 자궁동맥을 대치하는 외장골동맥에서 기시할 수 있는 측부순환동맥의 예로 잘 알려져 있으나(9), 본 증례에서는 원인대동맥과 별개로 변이동맥이 난소 및 자궁에 혈류를 공급하는 것으로 보였다(Fig. 2B). 난소동맥은 난소 혹은 자궁질환의 영향으로 비대해질 수 있다(5). 1,072명의 자궁동맥 색전술을 시행받은 환자를 연구한 바에 따르면 184(17.2%)명의 환자에서 적어도 한 개의 난소동맥은 커져 있었다(1). 또 다른 연구에 의하면 자궁동맥 색전술을 시행한 294명의 환자에서 75개의 비대해진 난소동맥이 보였으며, 이를 토대로 Pelage 등은 혈관조영술에서 동측의 자궁동맥의 크기가 작거나 없고 자궁이 조영되지 않는 경우에 추가적으로 난소동맥조영술을 하여 자궁으로의 난소동맥 측부순환 유무를 확인하여야 한다고 제안했다(3). 본 증례에서도 유사하게 우측 자궁동맥은 위축되어 있는 반면 우측 변이 난소동맥은 비대해져 있었고, 난소동맥 조영술에서 동측의 자궁 절반이 이 변이 동맥에 의해 혈류공급을 받고있는 것을 확인할 수 있었다. 난소동맥 발생의 변이에 대한 이해는 자궁동맥 색전술을 함에 있어서 측부순환을 평가하는데 매우 중요하다. 본 증례는 동측의 자궁동맥의 크기가 위축되어 있을 때, 동측 외장골동맥에서 기시하는 변이 난소동맥으로부터 자궁으로 들어오는 측부순환을 확인하여 성공적으로 색전술을 시행하였다는데 의의가 있다.
참고문헌
1. White AM, Banovac F, Yousefi S, Slack RS, Spies JB. Uterine fibroid embolization: the utility of aortography in detecting ovarian artery collateral supply. Radiology 2007; 244:291-298.
2. Razavi MK, Wolanske KA, Hwang GL, Sze DY, Kee ST, Dake MD. Angiographic classification of ovarian artery-to-uterine artery anastomoses: initial observations in uterine fibroid embolization. Radiology 2002; 224:707-712.
3. Pelage JP, Walker WJ, Le Dref O, Rymer R. Ovarian artery: angiographic appearance, embolization and relevance to uterine fibroid embolization. Cardiovasc Intervent Radiol 2003; 26:227-233.
4. Bensalah J, Dumousset E, Niro J, et al. Aberrant ovarian and uterine feeding from the renal artery at the end of gestation: two cases. J Vasc Interv Radiol 2010; 21:1911-1912.
5. Smoger DL, Kancherla V, Shlansky-Goldberg RD. Uterine fundal blood supply from an aberrant left ovarian artery originating from the inferior mesenteric artery: implications for uterine artery embolization. J Vasc Interv Radiol 2010; 21:941-944.
6. Ravery V, Cussenot O, Desgrandchamps F, et al. Variations in arterial blood supply and the risk of hemorrhage during percutaneous treatment of lesions of the pelviureteral junction obstruction: report of a case of testicular artery arising from an inferior polar renal artery. Surg Radiol Anat 1993; 15:355-359.
7. Cicekcibasi AE, Salbacak A, Seker M, Ziylan T, Buyukmumcu M, Uysal II. The origin of gonadal arteries in human fetuses: anatomical variations. Ann Anat 2002; 184:275-279.
8. Pelage JP, Cazejust J, Pluot E, et al. Uterine fibroid vascularization and clinical relevance to uterine fibroid embolization. Radiographics 2005; 25 Suppl 1:S99-117.
9. Saraiya PV, Chang TC, Pelage JP, Spies JB. Uterine artery replacement by the round ligament artery: an anatomic variant discovered during uterine artery embolization for leiomyomata. J Vasc Interv Radiol 2002; 13:939-941.
Fig. 1.
Fig. 1. T2-weighted sagittal MR image shows multiple submucosal and intramural uterine myomas, with the largest one measuring 6.1 x 4.2 x 5.9 cm.
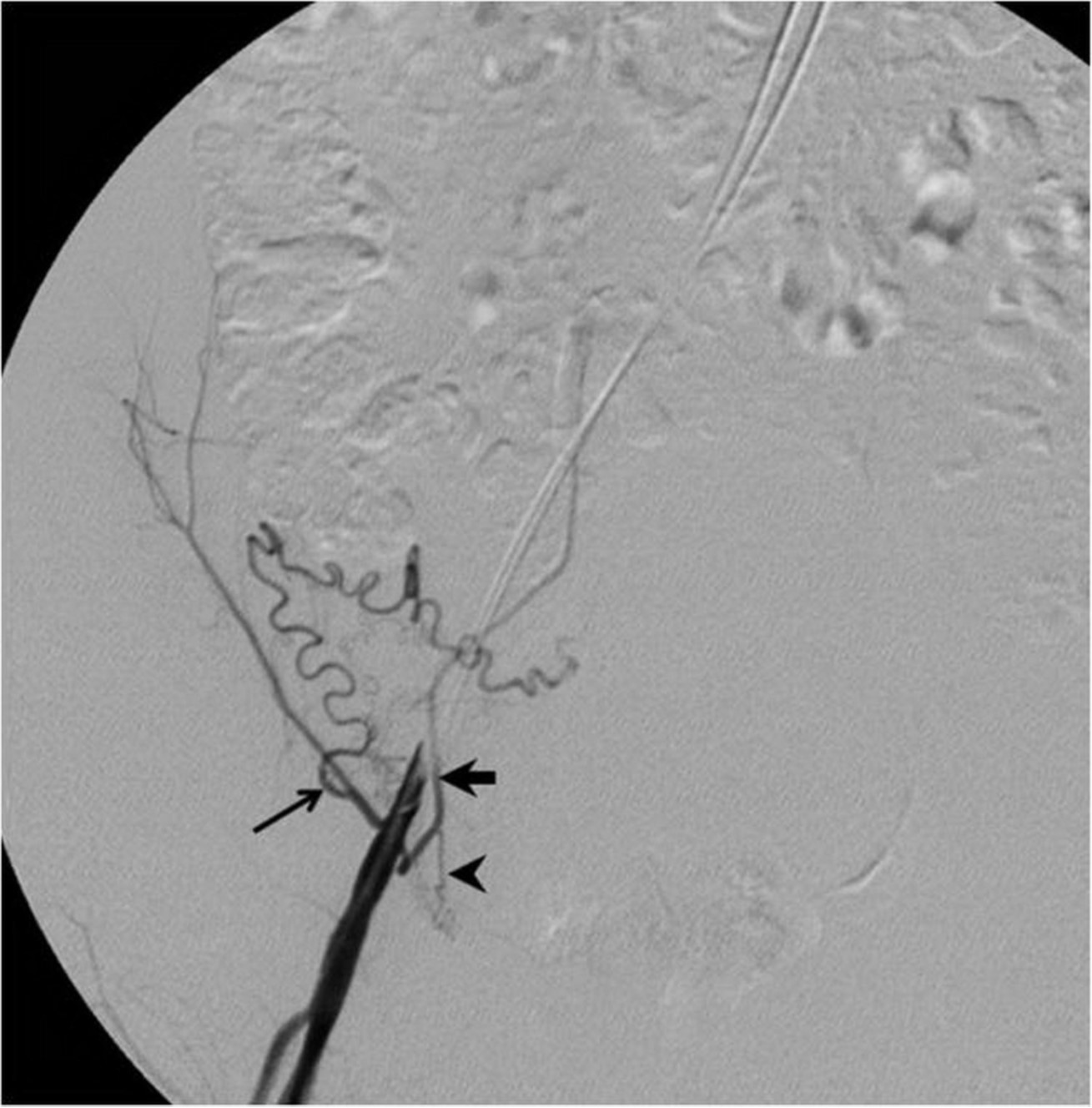
Fig. 2. A
Fig. 2A-C. Pelvic angiogram (A) shows the tortuous and dilated left uterine artery (arrow) and atrophy of the right uterine artery. An aberrant ovarian collateral (arrowhead) originates from the right external iliac artery. Selective right external iliac angiogram (B) reveals the aberrant ovarian collateral (thin arrow), right inferior epigastric(thick arrow), and right round ligament(arrowhead) arteries. Selective aberrant ovarian collateral angiogram (C) demonstrates that the collateral supplies blood flow to the right half of the uterus as well as the right ovary (arrow).
Fig. 2. B
Fig. 2A-C. Pelvic angiogram (A) shows the tortuous and dilated left uterine artery (arrow) and atrophy of the right uterine artery. An aberrant ovarian collateral (arrowhead) originates from the right external iliac artery. Selective right external iliac angiogram (B) reveals the aberrant ovarian collateral (thin arrow), right inferior epigastric(thick arrow), and right round ligament(arrowhead) arteries. Selective aberrant ovarian collateral angiogram (C) demonstrates that the collateral supplies blood flow to the right half of the uterus as well as the right ovary (arrow).
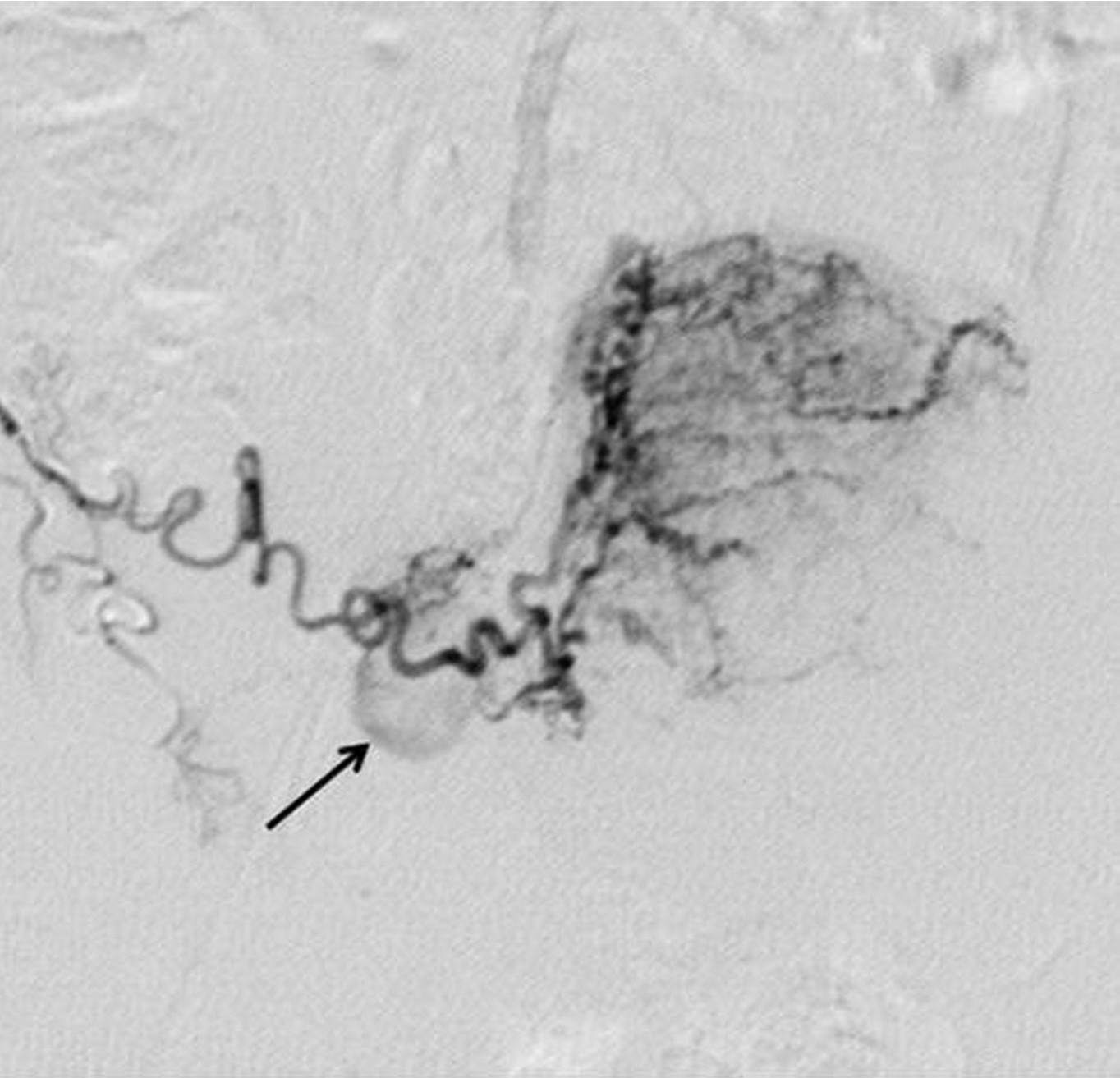
Fig. 2. C
Fig. 2A-C. Pelvic angiogram (A) shows the tortuous and dilated left uterine artery (arrow) and atrophy of the right uterine artery. An aberrant ovarian collateral (arrowhead) originates from the right external iliac artery. Selective right external iliac angiogram (B) reveals the aberrant ovarian collateral (thin arrow), right inferior epigastric(thick arrow), and right round ligament(arrowhead) arteries. Selective aberrant ovarian collateral angiogram (C) demonstrates that the collateral supplies blood flow to the right half of the uterus as well as the right ovary (arrow).
Fig. 3.
Fig. 3. T2-weighted sagittal MR image obtained 3 months after uterine artery embolization shows necrotic changes in most uterine myomas. The largest one shows 84.4% volume reduction.
Citations
Citations to this article as recorded by