중심단어
Veins, obstruction, Veins, brachiocephalic, Angioplasty
임상소견
만성신부전 환자로 2011년 6월 우측팔에 동정맥루(brachioaxillary arteriovenous graft) 수술 후 혈액투석을 받아오다 최근 우측 팔의 종창으로 내원함. 2011년 5월 우측 내경정맥에 영구 혈액투석 카테터 삽입력이 있음.
진단명
Occlusion of right brachiocephalic vein
영상소견
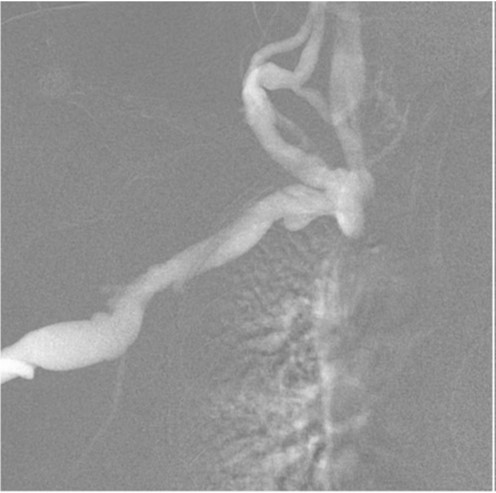
우측 중심정맥조영술에서 우측 상완두정맥(brachiocephalic vein)이 완전히 막혀있고 경정맥으로 여러 개의 측부혈관(collateral vessel)들이 관찰됨
시술방법 및 재료
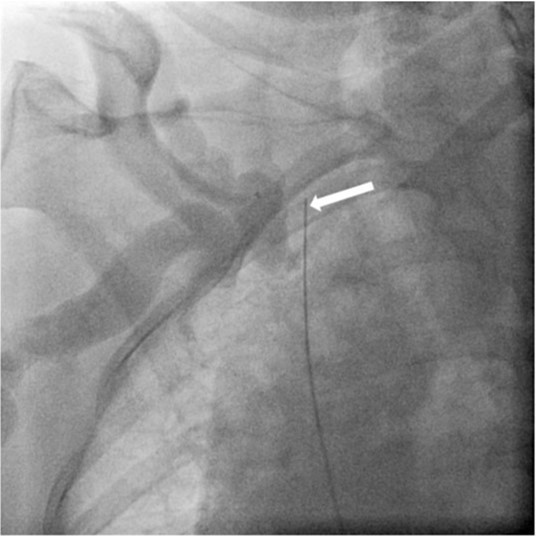
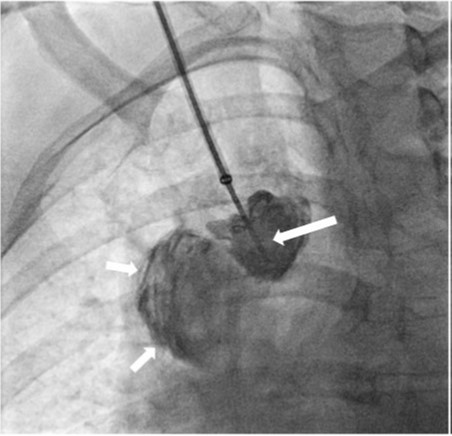
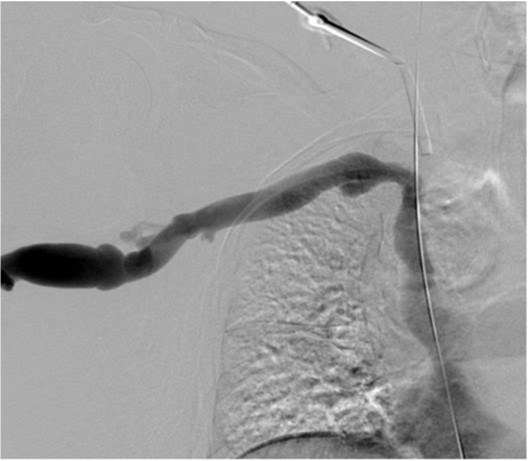
초음파 유도 하에 우측 팔의 동정맥루 graft를 천자한 후 정맥조영술을 시행하여 우측 상완두정맥의 폐색을 확인함(Fig. 1). 5Fr Cobra 카테터(Cook, Bloomington, IN, USA)와 친수성 0.035 inch 유도철사(Terumo, Tokyo, Japan)로 폐색부위의 통과를 시도하였으나 실패함. 우측 대퇴정맥을 천자하고9Fr 65cm sheath (Arrow, Deutschland, Erding, Germany)를 상대정맥까지 진입시킨 후 5Fr Davis 카테터를 통해 약 2cm 길이의 상완두정맥 폐색 부위를 확인함(Fig. 2). Davis 카테터와유도철사로 상대정맥에서 우측 상완두정맥으로 통과를 시도함. 유도철사의 soft tip 부분으로 시도하였을 때 통과가 되지 않아서 반대쪽 hard tip 부분으로도 통과를 시도 하였으나 실패함(Fig.3). 유도 철사의 soft tip 과 hard tip 양쪽 모두 사용 하여 통과를 시도하였으나 막힌 부위의 위쪽 부분은 앞쪽(anterior side of the body) 을 향하고 있고 아래쪽 부분은 뒤쪽(posterior side of the body)를 향하고 있어서 천자 방향을 맞추기 어려웠음(Fig. 3). 우측 내경정맥을 천자하고 5Fr sheath를 삽입함. Sheath를 통해서 5FrKumpe 카테터와 0.035 inch 유도철사로 위에서 아래 방향으로 폐색부위 통과를 시도함. Hard tip으로 시술 도중 폐색혈관 주위로 유도 철사가 천자되어서 조영제의 누출이 있었으나 천자부위 주에 국한되어 있었고 임상적으로 문제 있는 혈류역학적 변화는 오지 않았음. Kumpe 카테터와 유도철사로는 천자 방향을 맞추기가 어려워서TIPS set (Cook, Bjaeverskov, Denmark)를 사용하기로 함. 천자된내 경정맥에 10Fr introducer sheath를 삽입하고 20G Colapinto needle을 폐색부위까지 진입시킴. 양쪽에서 정맥 조영술을 시행하여 폐색된 부위의 위치와 길이를 여러 각도에서 정확히 파악한 후, 폐색 부위를 천자함(Fig. 4). 천자 후 Colapinto needle을 통해 유도철사를 상대정맥에 진입시킴. 대퇴동맥을 통하여 삽입된 snare 카테터(ev3, Plymouth, MA, USA)를 이용하여 대퇴정맥 밖으로 유도철사를 빼냄(through and through technique)(Fig 5). 유도 철사만 통과된 상태에서 천자부 주위에 여러번의 천자로 인한 조영제 누출이 있었으나 주출된 조영제의 양이 적었으며 천자부 주위에 국한되어 있었음. Tractogram시행시 조영제의 누출은 보이지 않아서 유도 철사 주위에 국한 되어 있어서 풍선확장술을 시행 하기로 함(Fig. 6).대퇴 정맥을 통해 유도철사를 0.035 inch Amplatz wire(Cook, Bjaeverskov, Denmark)로 교체하여 내경정맥까지 진입시킨 후 풍선카테터 (Bard, NJ, US)를 삽입함.천자된 통로를 따라 직경 6 mm에서부터 16 mm까지의 풍선카테터로 차례대로 풍선확장술을 시행함(Fig. 7). 시술 후 정맥조영술에서 폐색부위는 개통되어 원활한 혈류를 보였음(Fig. 8). 시술 후에 오른쪽 팔의 종창은 호전됨.
고찰
혈액투석환자에서의 중심정맥 협착 및 폐색은 본 증례에서처럼 일시적인 중심정맥 삽관에 따른 외상이 중요한 원인이 된다. 증상으로는 정맥압의 상승으로 팔에 심한 부종과 동통을야기하고, 일부는 얼굴과 목, 유방까지 부종이 발생한다. 이러한 중심정맥 협착은 혈액투석환자의 약 17%로 보고되고있다.
TIPS needle을 사용한 중심 정맥 폐색 재개통술은 2005년 Honnef 등이 처음 보고하였다. 당시 보고에서 는 왼쪽 상완두정맥 폐색이 있었으며, 유도철사와 21G needle로는 통과가 안되어 TIPS needle을 사용하였다. 이후 Athreya 등도 4명의 중심 정맥 폐색 환자에서 TIPS needle을 사용하여 재개통을 하였다.이렇게 유도철사나 일반적인 puncture needle이 폐색부위를 통과하지 못할 때 TIPS needle이 유용하게 쓰일 수 있다. 하지만 이 TIPS needle을 사용한 천자는 더욱 침습적이고 날카로운 천자이므로 그 이전에 대퇴정맥 접근을 통한 통과를 우선 시도하여야 한다.본 증례에서처럼 완전히 폐색된 중심 정맥을 천자할 때 주의사항으로는 여러 면에서 투시를 하여 예상 천자경로가 혈관 내에만 위치하도록 하여야 하며, 천자 후에는 pull-back 정맥 조영술을 시행하여 혈관 외 유출을 배제하여야 한다.
참고문헌
1. Haage P, Vorwerk D, Piroth W, Schuermann K, Guenther RW. Treatment of hemodialysis-related central venous stenosis or occlusion: results of primary Wallstent placement and follow-up in 50 patients. Radiology 1999;212:175-180.
2. Honnef D, Wingen M, Gunther RW, Haage P. Sharp central venous recanalization by means of a TIPS needle. Cardiovasc Intervent Radiol 2005;28:673-676.
3. Athreya S, Scott P, Annamalai G, Edwards R, Moss J, Robertson I. Sharp recanalization of central venous occlusions: a useful technique for haemodialysis line insertion. Br J Radiol 2009;82:105-108.
Fig. 1.
Fig 1. Venogram shows occlusion of the right brachiocephalic vein with multiple collaterals in the right neck.
Fig. 2.
Fig 2. Venogramshows short segmental occlusion of right brachiocephalic vein (long arrow) and vascular sheath (short arrow) within SVC which was inserted via right common femoral vein.
Fig. 3.
Fig 3. Fluoroscopic image shows guidewire passed across the obstructed segment. But the tip of the guidewire is positioned behind the right brachiocephalic vein (arrow).
Fig. 4.
Fig 4. Fluoroscopic image shows Colapinto needle punctured the right superior vena cava across the obstructed segment. The tip of the needle is facing back side of the body (long arrow). Confined contrast leakage is noted around the obstructed right brachiocephalic vein (small arrows).
Fig. 5.
Fig 5. Fluoroscopic image shows the guidewire passage the obstructed segment.
Fig. 6.
Fig 6. Tractogram via the vascular sheath shows no contrast leakage.
Fig. 7.
Fig 7. Fluoroscopic image showsdilatationof the occluded segmentby 16mmx4cm high pressure balloon.
Fig. 8.
Fig 8. Final digital subtraction venogram shows recanalization of the right brachiocephalic vein and disappeared collateral veins.
Citations
Citations to this article as recorded by