중심단어
Portal vein thrombosis, Portal hypertension, Stents, Bile duct Neoplasms
임상소견
고혈압과 고지혈증으로 약물 복용중인 환자로 1개월 전부터 시작된 황달 증상으로 촬영한 CT 및 MRI에서 총담관암 소견있어 총담관 및 간문맥 분절 절제 및 루엥 Y 간공장문합술 (Roux-en-Y hepaticojejunostomy) 시행 후 추적 검사로 시행한 도플러 초음파 및 CT 검사에서 문맥혈전증에 의한 문맥 협착 소견이 보임. 혈액 검사 상 헤모글로빈은 9g/dL로 저하, 화학 검사 상 AST/ALT 46/18 IU/L(정상치: 13-34/5-46 IU/L)로 AST의 경미한 증가, 총 빌리루빈 2.6mg/dL(정상치: 0.2-1.2 mg/dL)로 증가, 알부민 2.7g/dL(정상치: 3.3-5.3 g/dL)로 감소, 프로트롬빈 시간 11초, INR 0.97(정상치: 9.8-13.4초, 0.91-1.16 INR)로 정상 범위를 보였음.
영상소견
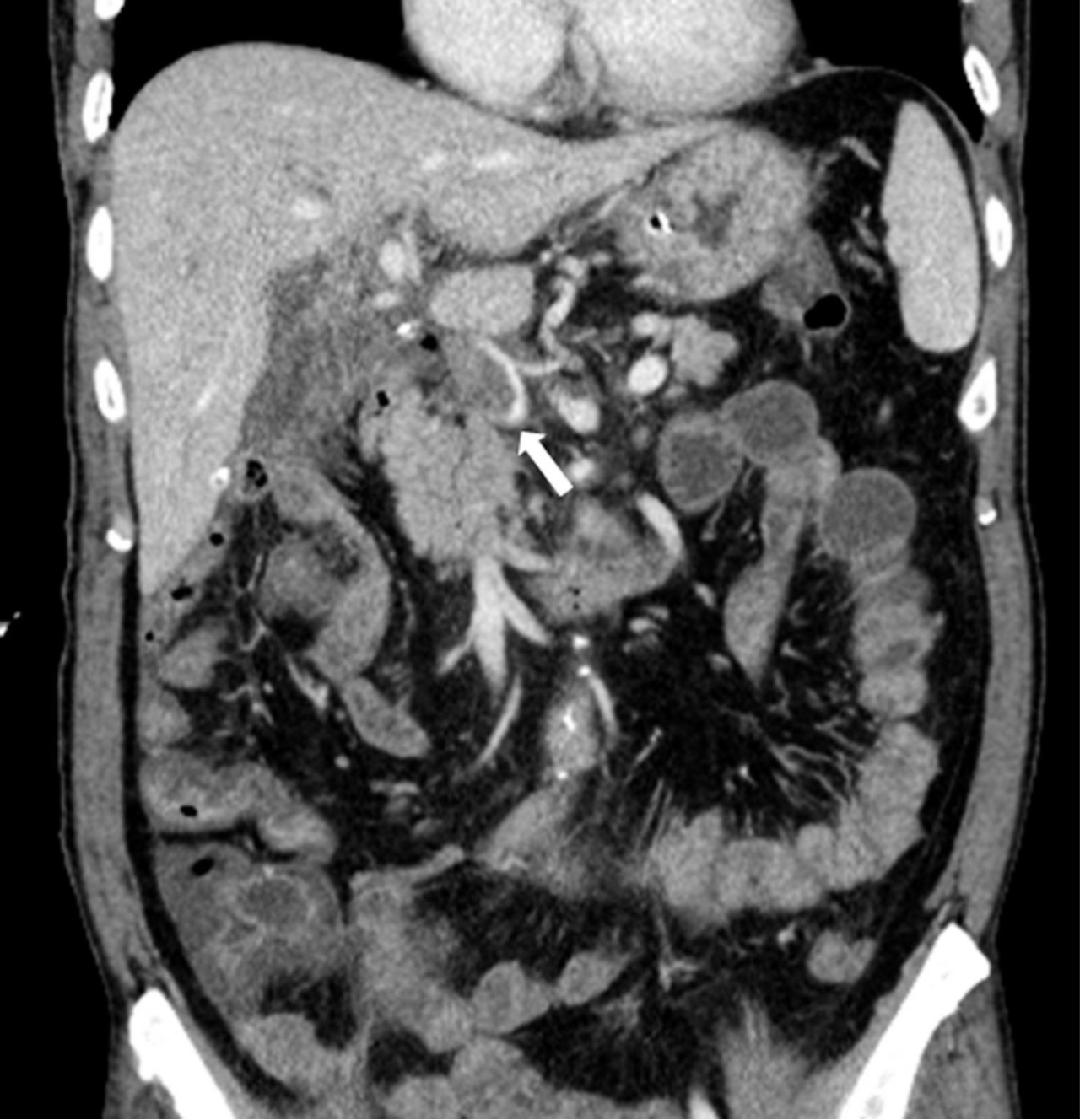
총담관과 간문맥 분절 절제 및 루엥Y 간공장문합술 시행 3일 후 촬영한 간 도플러 초음파에서 문맥의 혈류가 관찰되지 않았으며 주문맥을 비롯하여 양측 문맥에 동일에코의 결절들이 있어 혈전증으로 생각되었음. CT에서도 주문맥이 혈전에 의해 폐쇄되어 있어 원위부 문맥 혈류가 보이지 않았음(Fig. 1).
시술방법 및 재료
초음파 유도하에 간우엽 S6 담관을 천자하여 5Fr sheath(Terumo, Tokyo, Japan)를 삽입하고 5Fr KMP catheter(Cook, Bloomington, IN, USA)를 상장간막정맥에 위치시키고 시행한 직접 문맥조영술에서 주문맥에 부분적으로 폐쇄가 관찰되었고(Fig. 2a) 혈전으로 인한 폐쇄로 생각이 되었다. 7F McNamara sheath(Cook, Bloomington, IN, USA)를 삽입하여 흡인 혈전제거술을 수차례 시행하여 소량의 혈전이 흡인되었으나 문맥 혈류는 여전히 막혀있었음. 이에 12mm balloon(EverCross, EV3, Plymouth, MN, USA)으로 경피혈관확장술을 시행하였으나 이후 시행한 문맥조영술에서도 문맥 폐쇄 소견은 여전히 보였음. 이어 주문맥에 14x40mm 자가팽창형금속 스텐트(ELuminexx, Bard, Tempe, AZ, USA)를 설치하였으나 문맥에 폐쇄된 분절을 전부 포함할 수 없어 근위부에 12x4cm의 자가팽창형금속 스텐트(Zilver, Cook, Bloomington, IN, USA)를 추가로 설치하고 이후 12mm balloon으로 혈관확장술을 시행하였음. 마지막으로 시행한 문맥조영술에서 문맥은 개통되어 혈류는 회복되었으나 문맥 원위부에는 혈전이 일부 남아있었음(Fig. 2b). 천자한 통로는 histoacryl로 색전후 시술을 종료하였음. 간문맥 스텐트 설치 후 5일 뒤 시행한 CT에서 문맥 스텐트는 개통되어 있었고 조영 후 사진에서 문맥 혈류가 말초까지 가는 것을 확인할 수 있었음(Fig. 3). 환자는 이후 간기능 부전 및 문맥 고혈압의 증상 및 소견 없이 회복하여 퇴원하여 외래 추적 관찰 중임.
고찰
문맥고혈압 중 간외문맥 폐쇄로 인한 경우는 5-10% 정도를 차지한다. 간문맥 폐쇄 중에서도 양성 간문맥폐쇄는 문맥 주변 구조의 염증으로 인해 생기는데 이는 주로 담낭염, 담도염, 췌장염, 또는 간이나 담도계 수술후 문맥 주위로 유착이 생겨서 나타난다(1-3). 간암이나 췌장암, 담도암 등 악성 종양으로 인한 문맥 폐쇄의 경우는 15-24% 정도가 된다(4). 본 환자는 총담관과 간문맥 분절 절제 및 루엥Y 간공장문합술 3일 후에 문맥에 혈전증이 생긴 경우로 암의 재발로 인한 것은 아닌 것으로 사료되며 수술 후 합병증으로 나타난 양성간문맥 폐쇄의 증례로 사료된다.
수술 후 문맥 협착은 일반적으로 췌십이지장절제술 또는 간이식수술, 간엽절제술, 비장절제술 등과 같이 문맥을 절제한 후 다시 문합하는 수술의 합병증으로 나타난다(5). 이런 경우 수술 후 문맥 협착은 보통 일시적이거나 무증상으로 임상적으로 크게 의미를 두지 않는 경우도 많다(6). 그리고 문맥이 막혔다고 해서 반드시 증상이 나타나는 것은 아니므로 문맥 폐쇄로 인한 문맥 고혈압은 진단과 치료가 어려운 경우가 많다(7). 수술후 급성 문맥 혈전증으로 인한 증상은 비특이적인 복통부터 장간막 허혈로 인한 패혈증까지 다양하게 나타 날 수 있으므로 간담도계의 수술을 시행한 환자에서는 이를 염두에 두어야 한다(5). 급성 문맥 혈전증 발생 시 화학 검사 상 간기능검사는 보통 정상이나 아스파르테이트아미노전달효소(aspartate transaminase), 알칼리성 인산분해효소(alkaline phosphatase), 그리고 빌리루빈(bilirubin)이 경미하게 오르는 경우도 있다(8, 9). 문맥폐쇄가 만성적으로 진행되면 문맥고혈압이 올 수 있으며 이 경우 증상으로 가장 흔한 것은 식도나 위, 소장, 대장에서 생긴 정맥류로 인해 토혈을 하거나 혈변을 보는 것이며 이는 심각한 위장관계 출혈, 그리고 환자를 사망에까지 이르게 할 수도 있다(7). 문맥고혈압이 심해지면 간부전이 오고 복수가 차서 환자의 삶의 질에 영향을 미칠 수도 있다. 본 증례에서는 총담관 및 간문맥 분절 절제 및 루엥Y 간공장문합술 시행 후 환자가 특별한 증상을 호소하지 않았고 화학 검사 상에서도 수술 전과 뚜렷한 변화는 없었다. 다만 수술 시 간문맥을 단단연결(end to end anastomosis) 해줄 때 문맥의 길이가 짧아 당겨서 문합해야 했기에 합병증의 가능성이 있을 것으로 생각되어 수술의가 수술 후 단기간 내에 추적 검사로 초음파를 시행하여 문맥혈전증이 진단된 경우이다.
간담도계 수술 후 급성 문맥혈전증의 진단은 색 도플러(color Doppler)가 비침습적이고 저렴하며 높은 민감도(89-93%)와 특이도(92-99%)를 보이나 검사자 의존적이며 혈전이 장 가스에 가려 안 보이거나 에코가 발생하지 않는 경우 진단이 어렵다(5). 따라서 CT로 인한 간문맥혈전증의 진단이 높은 민감도(90%)와 특이도(99%)를 보이면서도 간문맥 해부학적 구조를 더 잘 볼 수 있는 방법이다(10).
문맥혈전증에 의한 문맥 폐쇄에 대한 치료는 명확히 정립되지는 않았지만 1990년대 들어 문맥 스텐트의 유용성이 대두되고 있다. Harville 등이 1991년 처음으로 문맥혈전증으로 정맥류 출혈이 있었던 환자에서 문맥스텐트를 시도하였고 문맥 혈류가 개통되고 위장관 출혈도 호전되는 성과를 얻었다(11). Yamakodo 등은 총 28개의 협착된, 12개의 폐쇄된 문맥 병변에 스텐트를 설치하여 평균 11.9 개월 동안 (2-61개월) 추적 관찰하여 60%의 스텐트가 재협착 없이 유지되었음을 발표하였다(4). Kim 등은 문맥 협착 환자에서 간문맥 스텐트를 설치한 경우 양성 협착으로 인한 경우가 췌담도계의 악성 종양 재발로 인한 문맥 협착보다 스텐트의 개통기간이 더 길었다고 보고하였다(12). 일반적으로 간문맥혈전증 진단 후 즉시 헤파린으로 항응고 치료를 해주어 혈전증의 진행을 방지해주는 것이 효과적이나 이는 50%의 환자에서만 완전히 혈전을 해소시켜주며, 만성문맥혈전증으로 문맥고혈압과 그 합병증이 오는 것을 방지하기 위해서는, 그리고 특히나 수술 직후에 문맥혈전증이 생긴 환자에서는 좀더 침습적인 치료가 필요하다(5). 인터벤션을 통해 혈전이 생긴 부위에 혈전용해(thrombolysis)를 해주는 것도 단기적으로 문맥 개통에 효과적일 수 있다(5).
간문맥 스텐트의 비적응증은 대표적으로 환자가 간부전에 빠져 있는 경우이다. 환자가 간부전에 빠져있으면 문맥에 스텐트를 설치해도 스텐트가 다시 막힐 확률이 높다(4). 혈전증이 간문맥뿐만 아니라 내장정맥(splanchnic vein)까지 침범한 경우도 문맥 스텐트는 적응증이 되지 않으며 악성 종양으로 인한 문맥 협착일 경우는 경동맥 항암치료(hepatic arterial infusion chemotherapy)와 방사선 치료가 환자의 생존을 더 늘려준다는 보고가 있다(13, 14). 간문맥 스텐트 후에는 천자부위의 통증, 일시적인 열, 간농양 등의 시술 관련 합병증이 발생할 수 있으며 스텐트 자체로 인해 혈전이 생길 수 있으므로 시술 후 항응고 치료를 하는 것이 필요하다(4).
본 증례와 같이 간문맥 혈전증으로 문맥 폐쇄가 온 환자에서 내장정맥의 손상이 없고 간부전이 오지 않았다면 간문맥 스텐트를 통한 치료가 문맥혈류를 개통시켜주고 문맥고혈압을 예방하여 환자의 삶의 질과 예후를 좋게 해준다.
참고문헌
1. Shan H, Xiao XS, Huang MS, Ouyang Q, Jiang ZB. Portal venous stent placement for treatment of portal hypertension caused by benign main portal vein stenosis. World J Gastroenterol 2005;11:3315-3318
2. Sarin SK, Agarwal SR. Extrahepatic portal vein obstruction. Semin Liver Dis 2002;22:43-58
3. Mitsunaga S, Kinoshita T, Kawashima M, Konishi M, Nakagohri T, Takahashi S, et al. Extrahepatic portal vein occlusion without recurrence after pancreaticoduodenectomy and intraoperative radiation therapy. Int J Radiat Oncol Biol Phys 2006;64:730-735
4. Yamakado K, Nakatsuka A, Tanaka N, Fujii A, Isaji S, Kawarada Y, et al. Portal venous stent placement in patients with pancreatic and biliary neoplasms invading portal veins and causing portal hypertension: initial experience. Radiology 2001;220:150-156
5. Thomas RM, Ahmad SA. Management of acute postoperative portal venous thrombosis. J Gastrointest Surg 2010;14:570-577
6. Hiraoka K, Kondo S, Ambo Y, Hirano S, Omi M, Okushiba S, et al. Portal venous dilatation and stenting for bleeding jejunal varices: report of two cases. Surg Today 2001;31:1008-1011
7. Ellis CM, Shenoy S, Litwin A, Soehnlein S, Gibbs JF. Effective endovascular stenting of malignant portal vein obstruction in pancreatic cancer. HPB Surg 2009;2009:426436
8. Sobhonslidsuk A, Reddy KR. Portal vein thrombosis: a concise review. Am J Gastroenterol 2002;97:535-541
9. Cohen J, Edelman RR, Chopra S. Portal vein thrombosis: a review. Am J Med 1992;92:173-182
10. Bach AM, Hann LE, Brown KT, Getrajdman GI, Herman SK, Fong Y, et al. Portal vein evaluation with US: comparison to angiography combined with CT arterial portography. Radiology 1996;201:149-154
11. Harville LE, Rivera FJ, Palmaz JC, Levine BA. Variceal hemorrhage associated with portal vein thrombosis: treatment with a unique portal venous stent. Surgery 1992;111:585-590
12. Kim KR, Ko GY, Sung KB, Yoon HK. Percutaneous transhepatic stent placement in the management of portal venous stenosis after curative surgery for pancreatic and biliary neoplasms. AJR Am J Roentgenol 2011;196:W446-450
13. Shibuya K, Nagata Y, Itoh T, Okajima K, Murata R, Takagi T, et al. Transcatheter arterial infusion therapy in the treatment of advanced pancreatic cancer: a feasibility study. Cardiovasc Intervent Radiol 1999;22:196-200
14. Bodner WR, Hilaris BS, Mastoras DA. Radiation therapy in pancreatic cancer: current practice and future trends. J Clin Gastroenterol 2000;30:230-233
Fig. 1. A
Figure 1. Contrast-enhanced CT scan following segmental resection of bile duct with Roux-en-Y hepaticojejunostomy and segmental resection of portal vein with end-to-end anastomosis. Both axial (A) and coronal (B) studies show a thrombus (arrows) in the narrowed main portal vein and peripheral portal flow is not seen.
Fig. 1. B
Figure 1. Contrast-enhanced CT scan following segmental resection of bile duct with Roux-en-Y hepaticojejunostomy and segmental resection of portal vein with end-to-end anastomosis. Both axial (A) and coronal (B) studies show a thrombus (arrows) in the narrowed main portal vein and peripheral portal flow is not seen.
Fig. 2. A
Figure 2. Portogram before the stent insertion (A) shows segmental obstruction in main portal vein and filling defect probably due to the thrombus. Portogram after portal vein stent demonstrates the patent stent and portal flow (B).
Fig. 2. B
Figure 2. Portogram before the stent insertion (A) shows segmental obstruction in main portal vein and filling defect probably due to the thrombus. Portogram after portal vein stent demonstrates the patent stent and portal flow (B).
Fig. 3. A
Figure 3. Contrast-enhanced CT study taken 5 days after the portal vein stent insertion. Stent is located in the main portal vein (arrows in A and D), with patent portal flow (B and C).
Fig. 3. B
Figure 3. Contrast-enhanced CT study taken 5 days after the portal vein stent insertion. Stent is located in the main portal vein (arrows in A and D), with patent portal flow (B and C).
Fig. 3. C
Figure 3. Contrast-enhanced CT study taken 5 days after the portal vein stent insertion. Stent is located in the main portal vein (arrows in A and D), with patent portal flow (B and C).
Fig. 3. D
Figure 3. Contrast-enhanced CT study taken 5 days after the portal vein stent insertion. Stent is located in the main portal vein (arrows in A and D), with patent portal flow (B and C).
Citations
Citations to this article as recorded by