중심단어
systemic artery to pulmonary artery malformation, fistula
임상소견
외부 병원에서 건강검진을 위해 시행한 전산화단층촬영(CT)에서 폐의 좌하엽에서 이상한 혈관성 병변이 발견되어 본원에서 CT혈관조영술을 추가적으로 시행하였음.
진단명
Systemic artery-pulmonary artery malformation
영상소견
전산화 단층촬영 (CT)에서 좌상폐의 설상엽에 동맥기에 동맥과 같은 정도로 조영증강되는 동맥류성 병변이 있으며, 굵어져 있는 좌상폐동맥의 분지, 양측 내유동맥 (left internal mammary artery), 8번 갈비뼈사이동맥 (intercostal artery), 좌측 아래횡경막동맥 (inferior phrenic artery)과 연결이 보임 (Fig 1). 각각의 체동맥에 대한 선택적 동맥 조영술에서 CT 소견에 부합하는 위치의 병변으로 향하는 구불구불한 동맥 원위분지가 확인되며, 특히 주 공급동맥인 좌측 내유동맥 조영술에서는 설상엽의 폐동맥 분지를 통해 좌측 주폐동맥까지 조영제가 역류하는 소견이 보임 (Fig. 2a~d).
Fig. 1.
A. A CT scan shows a pulmonary arterial aneurysm connected to multiple systemic arteries including both internal mammary arteries, left 8th intercostal artery and left inferior phrenic artery. B. A volume-rendering reformatted CT image shows a malformed pulmonary artery (arrow) and lingular pulmonary artery (arrowheads), which is connected to multiple systemic arteries including left internal mammary artery (open arrow) and left inferior phrenic artery (open arrowhead).
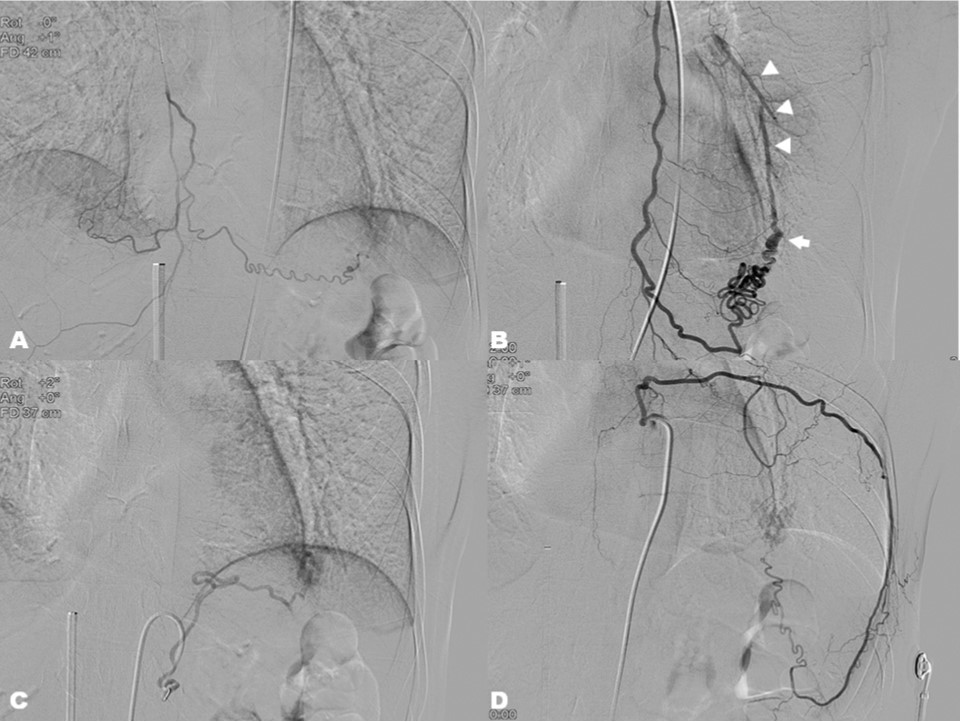
Fig. 2.
Selective angiographic for (A) right internal mammary artery, (B) left internal mammary artery, (C) left inferior phrenic artery, and (D) left 8th intercostal artery showed the fistulous connection to the malformed pulmonary artery (arrow) which is draining into lingular pulmonary artery (arrowheads).
시술방법 및 재료
우측 총대퇴정 맥을 통해 6Fr Arrow sheath를를 삽입하고 4Fr angled catheter (Davis, Cook, Indiana)를 이용하여 좌측 주폐동맥을 선택한 후 pigtail catheter를 이용하여 폐동맥조영술을 시행하였으나 설상엽의 폐동맥 분지는 조영되지 않음 (Fig 3a). 이는 체동백-폐동맥 간 연결을 통해 혈류의 방향이 역전되어서 생긴 현상으로 판단됨. 이에 RAO 45도에서 좌측 내유동맥 조영술 DSA 영상에서 설상엽 폐동맥의 분지가 보이는 시기의 영상을 Smart roadmap 기능 (Allura Xper, Philips Medical, Ne比terlaM)을 이용하여 투시 영상에 중첩(overlay)시킨 후 주폐동맥에 위치한 유도철사 (0.035” hydrophilic guidewire, Terumo, Tokyo, Japan)와 Davis catheter를 조작하여 설상엽 폐동맥 분지를 선택하는데 성공하였음 (Fig 3b). 이후 동맥 malformation을 다수의 detachable coil (018” Interlcok detachable coil 3mmx6cm, 3mmx12cm, 4mmx8 cm, 5mmx8 cm, 6mmx10cm, Boston Scientific, Natick, Massachusetts) 과 microcoil (018” Micronester 4mmx14cm, 7mmx14cm)을 이용하여 접근 가능한 가장 먼 유입부에서부터 동맥류성 변화를 보이는 부위까지 색전술을 시행하였음 (Fig 4). 이후 양측 내유동맥의 분지를 각각 2.0Fr Progreat microcatheter (Terumo)을 이용하여 초선택한 후 n-butyl cyanoacrylate 0,5cc와 Lipiodol (Guerbet, France) 2.5cc의 혼합물을 이용하여 색전술을 시행하였음 (Fig 5a-b). 좌측 8번째 갈비뼈사이동맥과 좌측 아래횡경막동맥은 기시부의 급격한 각도 변화로 microcatheter가 진입되지 않아서 polyvinyl alcohol particle (Contour 45-150mhi, Boston scientific)을 이용하여 색전술을 시행하였음 (Fig 5c-d). 시술 3개월 후 추적관찰을 위해서 흉부촬영에서 해당위치에 coil과 Lipiodol이 변화없이 안정적으로 보이고 있음.
Fig. 3.
A. The systemic artery to pulmonary artery malformation was not visualized in the left pulmonary arteriography due to the reversed flow direction. B. A roadmap of the digital subtraction angiography performed at left internal mammary artery (open arrow) was overlayed on screen to guide the catheter and wire into lingular pulmonary artery (arrowheads) and the malformed pulmonary artery (arrow).
Fig. 4.
Multiple microcoils were placed to obligate the aneurysmal space and to retard the systemic arterial flow into the pulmonary artery.
Fig. 5.
Selective embolizations for (A) right internal mammary artery, (B) left internal mammary artery, (C) left inferior phrenic artery, and (D) left 8th intercostal artery were performed to occlude systemic arterial inflow into the malformation.
고찰
체동맥과 폐동맥 사이의 이상 연결은 폐실질이 파괴되는 폐결핵 또는 기관지확장증에 동반된 단락(shunt)의 형태로 나타난다. 본 증례에서와 같이 거시적인 크기의 동맥간 직접 연결은 매우 드물다. 그 원인은 선천적 또는 흉막- 폐의 감염증 등으로 추정하고 있다. 이러한 병변이 발견되었을 때 시행하는 목적은 폐동맥 고혈압 및 심부전의 발생을 방지하고 동맥류의 파열에 의한 출혈을 예방하는 것이다. 기존에는 주로 해당엽을 절제하는 수술적 치료가 이루어졌으나, 최근 혈관내 인터벤션 치료가 발달하면서 체동맥 및 폐동맥 색전술을 이용하여 성공적으로 치료한 증례들이 보고되고 있다. 폐동정맥기형은 페동맥과 폐정맥 사이의 직접적인 연결이 있는 것으로 폐동정맥기형의 70%는 hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu증후군)와 관련이 있다. 폐동정맥 기형에 체동맥이 혈류를 공급하는 기전은 정확히 알려진 바가 없으나, 수술이나 경피적 치료에 대한 반응으로 생길 수도 있고, 폐나 흉막의 염증이나 감염에 의한 휴유증일 수도 있다. 본 증례는 체동맥과 폐동맥 사이의 이상 연결만 보이고, 폐정맥과의 연결이 없어서 폐동정맥기형과는 구분이 된다.
참고문헌
1. Serdar Geyik, Kivilcim Yavuz, Frederick S. Keller. Unusual Systemic Artery to Pulmonary Artery Malformation Without Evidence of Systemic Disease, Cardiovasc Intervent Radiol 2006; 29: 897-901
2. Sagara K, Miyazono N, Inoue H, Ueno K, Nishida H, Nakajo M. Recanalization after coil embolotherapy of pulmonary arteriovenous malformations. AJR Am J Roentgenol 1998; 170: 727-730
3. Laffey KJ, Thomashow B, Jaretzki A, Martin EC. Systemic supply to a pulmonary arteriovenous malformation: A relative contraindication to surgery. AJR Am J Roentgenol 1985; 145: 720-722
4. Wispelaere JF, Trigaux JP, Weynants P, Delos M, Coene BD. Systemic supply to a pulmonary arteriovenous malformation: Potential explanation for recurrence. Cardiovasc Intervent Radiol 1996; 19:285-287
5. Lee DW, White Rl, Egglin TK, et al. Embolotherapy of large pulmonary arteriovenous malformations: Long-term results. Ann Thorac Surg 1997; 64: 930-940
6. Mager JJ, Oertoom TTC, Blauw H, Lammers JWJ, Westermann CJJ. Embolotherapy of pulmonary arteriovenous malformations: Long-term results in 112 patients. J Vase Interv Radiol 2004; 15: 451-456
Citations
Citations to this article as recorded by