중심단어
portal vein, stent-graft, jejunalvarix, embolization
임상소견
췌관 팽대부암으로 2011년 4월 21일 유문보존췌십이지장절제술을 시행받고 총간동맥 가성동맥류로 색전술을 시행한 과거력이 있음. 복부불편감과 구토, 설사가 발생하여 시행한 전산화 단층촬영에서 주간문맥의 폐색과 간-공장문합부위에 정맥류 출혈이 의심되었다.
진단명
Jejunalvarix bleeding
영상소견
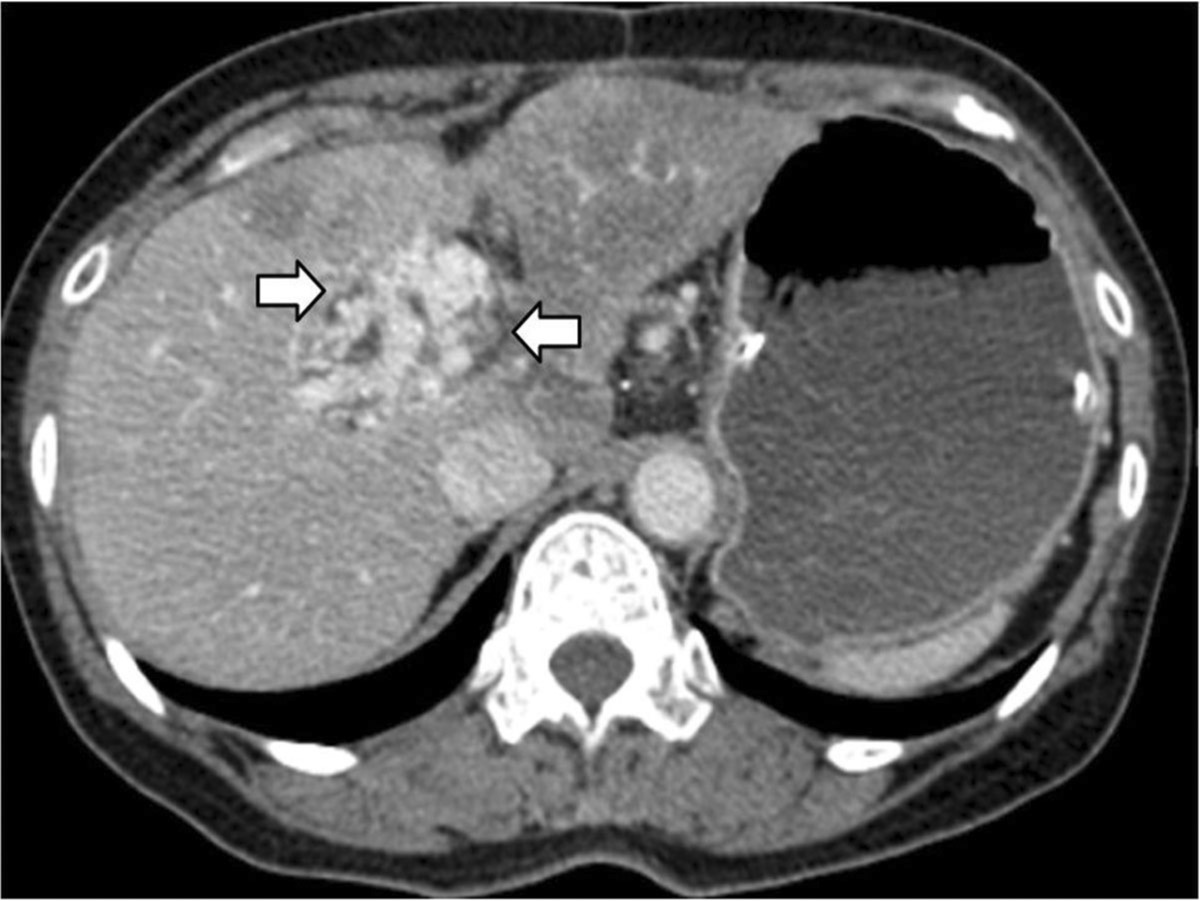
조영증강 복부 전산화단층촬영에서 간-공장 문합부위에 공장정맥류가 확인되었고 주문맥은 폐색으로 인해 관찰되지 않았다 (Fig 1).
Fig. 1.
Fig. 1. Contrast enhanced CT scan of abdomen demonstrate jejunalvarix in hepaticojejunostomy site (arrows) and nonvisualization of the main portal vein.
시술방법 및 재료
초음파 유도하에 chiba needle을 이용하여 percutaneous transhepatic approach를 통해 우측간문맥을 천자하여 8Fr sheath를 삽입하였다. 좁아져 있는 주간문맥을 Kumpe catheter, microcatheter & wire를 이용하여 통과하는데 성공하였다. 환자는 이전에 수술 후 발생한 총간동맥의 가성동맥류에 대해 coil 색전술을 시행받았었다 (Fig 2A). 상장간막정맥에서 시행한 혈관조영술상 주간문맥은 폐쇄되어 있고 상장간막정맥에서 분지하는 공장 정맥류가 확인되었다(Fig. 2B).
주간문맥의 협착에 대해서 3mmx15cm, 5mmx4cm balbon catheter를 이용하여 순차적으로 혈관성형술을 시행하였다. 주간문맥에 풍선성형술을 하고 시행한 비장정맥 혈관조영술상, 주간문맥의 협착과 공장정맥류가 여전히 남아있었다(Fig 2C). 이에 Viabahn 8mmx5cm stent-graft를 거치하고 stent-graft 내부를 8mmx4cm baltoon catheter를 이용하여 혈관성형술을 시행하였다. 이후 시행한 비장정맥 혈관조영술에서 stent-graft 내부로의 혈류 및 비장정맥의 배수, 좌측간문맥으로의 혈류가 모두 원활함을 확인하였다(Fig 2D). 그러나, 상장간막정맥과 주간문맥 합류 부위에 국소적인 협착이 관찰되었고 여전히 공장 정맥류가 확인되었다(Fig 2E). 이에 Kumpe catheter, microcatheter를 이용하여 상장간막정맥으로부터 분지하는 공장 정맥류를 선택한 후, glue와 lipiodol 1:5 mixture를 이용하여 색전술을 시행하였다 (Fig 2F). 색전술 후 시행한 문맥조영술상 주간문맥에 거치된 stent-graft와 상장간막정맥 합류 부위에 협착이 남아 있어 Zilver 8mmx4cm stent를 거치한 후 8mmx5cm balloon catheter를 이용하여 혈관성형술을 시행하였다. 이후 Kumpe catheter를 이용하여 상장간막정맥에서 시행한 문맥조영술상 공장 정맥류는 대부분 폐색되었고 주간문맥에 거치된 stent-graft를 통한 혈류가 원활함을 확인하였다(Fig 2G). 우측간문맥과 percutaneous transhepatic tract을 glue와 lipiodol 1:1 mixture를 이용하여 색전술을 하고 시술을 종료하였다.
Fig. 2.
A. After the portal van puncture under ultrasonic and fluoroscopic guidance, successful navigation of the occluded main portal vein was achieved using microcatheter & wire. She had undergone coil embolization (arrow) of the common hepatic artery due to pseudoaneurysm at the stump of gastroduodenal artery.
B. Superior mesenteric venography shows total occlusion of the main portal van (arrow) and extensive jejunalvarix (arrowheads).
C. Splenic vaiography, after 5mm-size balloon angioplasty for occluded main portal vein, demonstrates residual narrowing of the main portal vein with still renained jejunalvarix.
D. Splenic venography after stent-graft placement shows patent main PV stent-graft with well drainage of the splenic vein and good blood flow through the left portal vein.
E. Superior mesenteric venography after stent-graft placement shows patent main PV but, residual focal stenosis at confluent of SMV and MPV (arrow). Extensive jejunavarix was also noted.
F. Selective angiography of the jujunal vein shows extensive jejunalvarix. Jejunal varix embolization was performed using glue & lipiodol 1 : 5 mixture.
G. Final Superior mesenteric venography, after bare stent insertion for residual stenosis at confluent of SMV and MTV (arrow), demonstrates widely patent MTV stent and complete occlusion of the jgunalvarix without residual contrast filling within the varices.
고찰
후천적 간문맥 협착 또는 폐색은 간이식수술 후에 가장 흔히 발생한다. 간이식수술과 관련 없는 후천적 간문맥 협착의 원인으로는 췌장염, 간담췌종양의 간문맥 침범, 수술 합병증 등이 있다. 후천적 간문맥 협착 후 이차적인 영향으로 간문맥 고혈압이 발생할 수 있고, 이로 인해 정맥류가 식도, 위, 십이지장, 소장에 발생할 수 있다. 이렇게 발생한 정맥류가 위장관 출혈을 일으켜 사망에 이를 수 있고, 문맥고혈압은 반복적인 복수의 발생으로 환자의 삶의 질을 저하시키는 요인이 되기도 한다.
후천적 간문맥 협착 또는 폐색에 대한 혈관내 치료법으로 stent 삽입과 혈관성형술을 시행할 수 있고, 동시에 동반된 정맥류에 대해서는 색전술을 시행할 수 있다. 이러한 혈관중재술은 시술관련 합병증의 발생률이 낮아 안전하게 시행할 수 있다. 또한 다른 치료법의 선택이 없는 환자에서 완화목적으로도 안전하게 시행할 수 있고, 시술 후 문맥고혈압으로 인한 증상들을 효과적으로 조절할 수 있는 치료방법이다.
본 증례에서는 주문맥이 long segmental occlusion의 소견을 보이며, CT에서 주문맥이 obliteration되어 있어 과도한 혈관성형술을 시행할 경우 혈관의 파열될 위험이 있을 것으로 판단하였다. 따라서 5mm balloon을 사용하여 주문맥을 약간 확장한 후 stent-graft를 삽입하였다. 주문맥의 길이(상장간맥정맥과 비장정맥의 합류부 지점부터 좌-우 간문맥의 분기점까지의 길이)가 5cm으로 측정되어 5cm길이의 Viabahn stent-graft를 사용하였다.
참고문헌
1. Woodrum DA, Bjarnason H, Andrews JC. Portal vein venoplasty and stent placement in the nontransplant population. J Vasc Interv Radiol. 2009;20(5):593-9
2. Shan H, Xiao XS, Huang MS, Ouyang Q, Jiang ZB. Portal venous stent placement for treatment of portal hypertension caused by benign main portal vein stenosis. World J Gastroenterol. 2005 Jun 7;11(21 ):3315-8.
3. Novellas S, Denys A, Bize P, Brunner P, Motamedi JP, Gugenheim J, Caroli FX, Chevallier P. Palliative portal vein stent placement in malignant and symptomatic extrinsic portal vein stenosis or occlusion. Cardiovasc Intervent Radiol. 2009 May;32(3):462-70
4. Yamakado K, Nakatsuka A, Tanaka N, Fujii A, Isaji S, Kawarada Y, Takeda K. Portal venous stent placement in patients with pancreatic and biliary neoplasms invading portal veins and causing portal hypertension: initial experience. Radiology. 2001 Jul;220(1 ):150-6.
5. Lee JY, Song SY, Kim J, Koh BH, Kim Y, Jeong WK, Kim MY. Percutaneous transsplenic embolization of jejunalvarices in a patient with liver cirrhosis: a case report. Abdom Imaging. 2013 Feb;38(1):52-5
Citations
Citations to this article as recorded by