중심단어
small for size syndrome, embolization of portocaval shunt, vascular plug
임상소견
B-viral hepatitis로 HCC 가 발생하여 LDLT 수술을 받은 환자로 수술 전 측정한 Graft-to- recipient body weight ratio(GRWR)가 약 0.59로 측정되었다. SFSS를 예방하기 위해서 수술 시, left portal vein을 inferior vena cava에 연결하여 hemiportocaval shunt를 만들었다. 수술 후 약 한달 뒤에 hemiportocaval shunt embolization이 의뢰되었다. Embolization이 의뢰될 시기의 혈액검사에서 ALT가 상승되어 있었지만 (ALT: 100 U/L), 다른 검사 결과들은 모두 정상치로 나타나 간 기능은 정상이었다 (total bilirubin : 1.0 mg/dl, AST : 29 U/L, INR : 1.06, Prothrombin time : 13.7sec).
영상소견
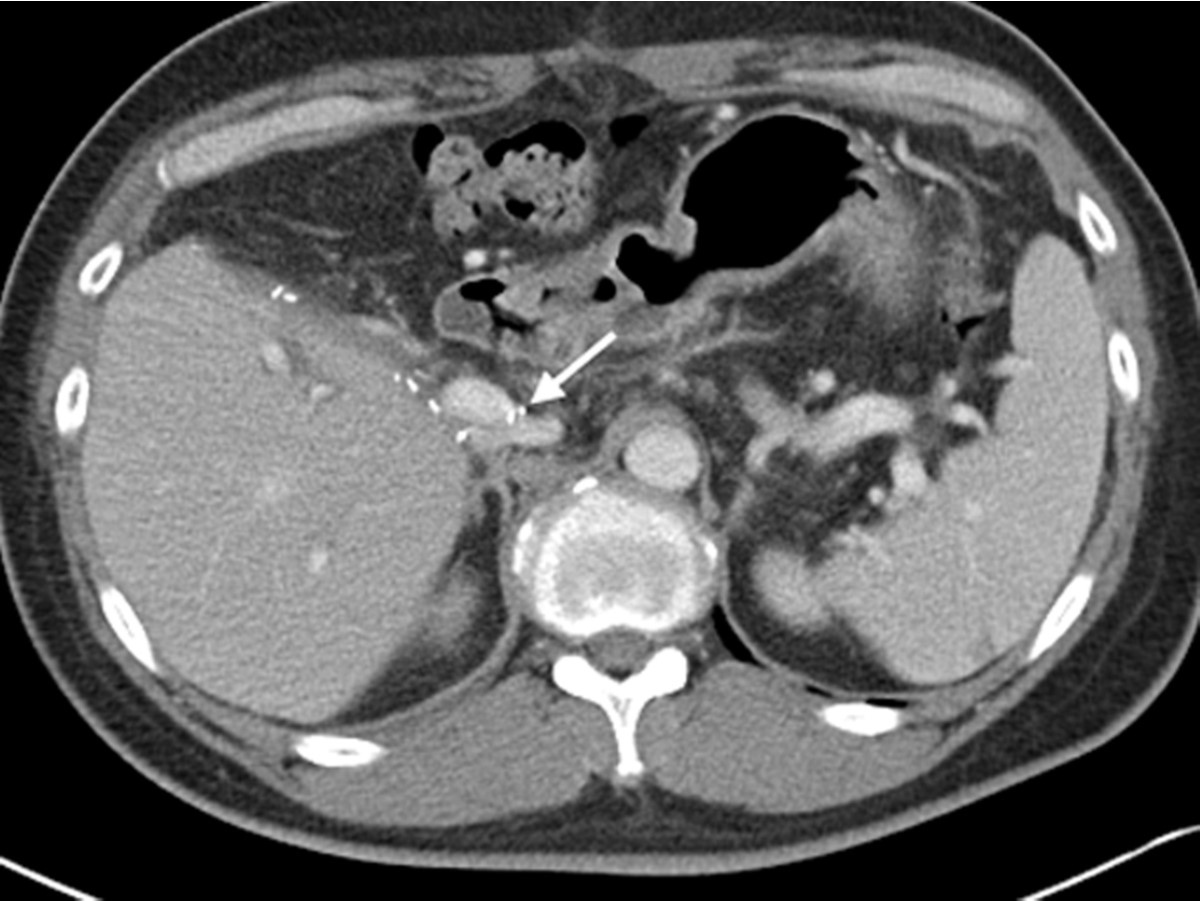
수술 전 CT에서 liver cirrhosis와 함께 S6에 1.9cm 크기의 HCC가 관찰되어 LDLT를 받았다. 수술 14일 후 시행한 abdomen enhanced CT에서 left portal vein은 IVC와 연결되어 있고 (Fig. 1), right portal vein은 graft liver에 연결되어 있어 hemiportocaval shunt를 확인 할 수 있었다. Hepatic perfusion defect 나 ascites 등은 관찰되지 않았다.
Fig. 1.
Fig. 1. Portal phase of abdomen CT, after LDLT with haniportocaval shunt formation shows left portal vein connected to inferior vena cava (arrow). Note the metallic surgical materials around the shunt.
시술방법 및 재료
초음파 유도하에 right portal vein peripheral branch를 22G needle로 puncture 하고, portal venography를 시행하여 left portal vein과 IVC의 연결을 확인하였다. 이 때 portocaval shunt는 잘 유지되어 portal flow가 IVC쪽으로 빠져나가는 것이 확인되었다. Embolization 전에 main portal vein에서 pressure를 측정한 결과, 18mmHg였으며, pressure가 20mmHg이하로 유지되고 있어 embolization을 진행하기로 하였고, portal venography에서 shunt의 직경은 13.4 mm, 길이는 17.5 mm로 측정되어(Fig.2), 직경 16 mm 크기의 Amplatzer® Vascular Plug II(AVP II, St. Jude Medical, MN, US)를 사용하기로 결정하였다. 0.035 inch hydrophilic guide wire(Radifocus® Guide wire M, Terumo, Japan)를 사용하여 wire를 IVC로 넘긴 뒤, 9F guiding catheter(RDC, Cordis, Johnson & Johnson Medical, US)를 portocaval shunt 내부로 전진하여 tip을 IVC쪽까지 넘겨둔 후, 이를 따라 shunt 부위에 16mm 직경의 Amplatzer® Vascular Plug II (AVP II, St. Jude Medical, MN, US)를 삽입하여 guiding catheter tip의 위치를 빼면서 plug의 설치 위치를 조절하여 shunt 내부에 deploy한 뒤, detach를 하지 않은 상태에서 약10분 정도 기다려 portocaval shunt의 flow가 멎는 것을 확인하였다. 완전히 flow가 막힌 것을 확인 한 다음, plug의 위치가 portal vein과 IVC 양쪽 모두로 protrusion이 없음을 확인하고 vascular plug를 detach 하였다(Fig, 3). 시술 후 시행한 마지막 angiogram에서 portocaval shunt는 완전히 막혔고, embolization 시행 후 측정한 main portal venous pressure는 25 mmHg 였다. Puncture tract은 gelfoam으로 packing 하여 bleeding을 방지하였다. Shunt embolization 시행 6개월 뒤에 시행한 abdomen enhanced CT에서 embolization은 잘 유지되어 left portal vein과 IVC는 잘 분리되어 있었다(Fig. 4).
Fig. 2.
During shunt embolization, main portal venography shows a patent portocaval shunt (arrows). The diameter and length of the portocaval shunt were each 13.4mm and 17.5mm.
Fig. 3.
After deployment of vascular plug (arrows) at the portal side of portocaval shunt demonstrates no flow from portal vein to inferior vena cava.
Fig. 4.
6 months after embolization of hemiportocaval shunt using vascular plug. Follow up enhanced abdomen CT shows vascular plug (arrows) between portal vein and inferior vena cava.
고찰
Small-for-size syndrome LDLT시에 partial liver graft가 recipient의 functional demand를 수용하지 못하여 coagulopathy, ascites, cholestasis와 encephalopathy등의 liver failure가 발생하는 증후군으로 일반적으로 Graft-to-recipient body weight ratio (GRWR)가 0.8 미만인 경우에 발생할 수 있는 것으로 보고되었다(1, 2). SFSS 발생에는 graft volume 뿐만이 아니라 다른 여러 가지 요인이 관여하는 것으로 알려져 있는데, graft liver에 steatosis와 같은 기저질환이 있거나, portal hyperperfusion, arterial hypoperfusion 등이 있는 경우, recipient가 수술 전 portal hypertension이 있거나 Child-Pugh Score가 B 이상인 경우에 SFSS가 호발하는 것으로 알려져 있다 (1-3). 본 증례의 환자는 LDLT 전 Child-Pugh score는 A였고, 술 후 portal hypertension은 없었으나, graft size가 작아 SFSS 발생 가능성이 있을 것으로 예상되는 환자였다.
SFSS의 치료에 사용되는 시술은 splenic artery modulation과 portocaval shunt를 시행해 portal pressure gradient를 줄여주는 것이 있다(1, 4, 5). 여러 연구에서 LDLT 수술 후 TIPS를 시행하거나 LDLT 수술 시 portocaval shunt를 만들어 SFSS를 예방하는 방법이 보고되었다(3, 4, 6). 그러나 Shunt를 만들어 SFSS를 예방하거나 치료하게 되면 이식된 간으로 혈류 공급이 줄어들어 chronic ischemia를 초래하게 되고, 따라서 graft의 long term viability가 좋지 않으므로 이러한 shunt는 pcrtal flow를 적정수준으로 유지할 수 있는 시기에 막아주는 것이 필요하다(1-3, 6). 한 논문에서는 IVC에 stent graft를 deploy하여 portocaval shunt를 막고, 1년 추적관찰에서 liver function이 정상으로 유지되었다고 보고 하였다 (7). 그러나 stent graft를 사용한 경우 stent patency가 장기간 보장되지 않기 때문에, 본 증례의 환자는 hemiportocaval shunt 수술 후 약 25 일째에 vascular plug를 이용하여 shunt embolization을 시행하였다. Yagi 등이 2005년 발표한 논문에 따르면 수술 후 early period에 portal pressure가 20 mmHg 이상인 경우 hepatocyte growth factor가 증가하고 graft hypertrophy가 빨리 일어나는 반면에 SFSS 또한 발생률이 높아질 수 있다고 하였다 (8). 반면, Ogura 등이 발표한 대규모 연구(n = 134)에서는 수술 후,portal pressure가 15 mmHg 이하로 적절히 조절되어야 LDLT 환자에게서 좋은 결과를 기대할 수 있다고 보고하여 (9), 아직까지는 liver transplantation을 집도하는 외과의들 사이에서 도 정확한 pressure에 대한 동의가 이루어지지 않고 있다. 본 증례의 환자는 embolization 전에 시행한 portal pressure가 18mmHg로 측정되어 Yagi 등의 논문을 참고하여 shunt embolization을 결정하였다. Shunt embolization 후에 portal pressure가 25 mmHg로 측정되어 기대했던 정도보다 높았지만, 시술 후 추적 기간 동안 혈액검사 상 total bilirubin 과 AST/ALT는 지속적으로 정상으로 나타나 SFSS 발생 없이 graft liver의 기능이 온전한 것을 알 수 있었다.
LDLT 후, shunt embolization을 시행하는 portal pressure의 기준에 대한 이견이 많은 것과는 달리, 많은 논문에서 수술 후 30일 이내의 초기에는 portal pressure가 높은 것이 좋지 않은 결과를 초래할 수 있다는 것에는 동의하고 있다(7-9). 본 증례에서는 portal pressure가 높지는 않았지만, shunt에 의해서 장기적으로 발생할 수 있는 portal flow steal phenomenon을 방지하기 위해서 약 1달 정도 지난 뒤에 shunt embolization을 시행하였는데, shunt embolization을 시행하는 보다 적절한 시기에 대해서는 더 많은 연구가 필요하다. 또한 본 증례와 같이 portal pressure가 20 mmHg 이하로 유지되고 있었던 경우에도 예방적인 embolization이 필요한 지에 대해서는 추가적인 연구가 필요할 것으로 생각된다. 또한 portovacal shunt는 shunt의 길이와 직경에 따라 embolization material의 선택이 달라지게 되며, 대부분은 길이가 짧아 coil과 같은 material은 shunt를 막는데 안전하게 사용하기 어렵다. 따라서 위치를 정밀하게 조절할 수 있는 Amplatzer vascular plug 이 좋은 대안이 될 수 있으며 shunt의 길이가 더 짧은 경우에는 본 증례와 같은 type II vascular plug보다는 type I vascular plug이 더 좋을 수도 있다.
Portocaval shunt embolization의 long-term follow up 연구가 없으므로 complication 발생 유무와, shunt embolization이 실제 liver graft의 outcome과 survival에 어떤 영향을 주는지는 추가적인 연구가 필요하다.
참고문헌
1. Gonzalez HD, Liu ZW, Cashman S, Fusai GK. Small for size syndrome following living donor and split liver transplantation. World J Gastrointest Surg 2010 Dec 27;2(12):389-94
2. Dahm F, Georgiev P, Clavien PA. Small-for-size syndrome after partial liver transplantation: definition, mechanisms of disease and clinical implications. Am J Transplant 2005 Nov;5(11):2605-10
3. Troisi R, Ricciardi S, Smeets P, et al. Effects of hemiportocaval shunts for inflow modulation on the outcome of small-for-size grafts in living donor liver transplantation. Am J Transplant 2005 Jun;5(6):1397 -404
4. Ji-wei H, Lu-nan Y, Zhe-yu C, et al. Hemi-portocaval shunt: A simple salvage maneuver for small-for-size graft during living donor liver transplantation. Chin Med J2011;124(14):2231-3
5. Tanaka K, Ogura Y. "Small-for-size Grat" and “Smallfor- size Syndrome" in Living Donor Liver Transplantation. Yonsei Med J 2004;45(6): 1089-94
6. Xiao L, Li F, Wei B, Li B, Tang CW. Small-for-size syndrome after living donor liver transplantation: successful treatment with a transjugular intrahepatic portosystemic shunt. Liver Transpl 2012 Sep;18(9):1118-20
7. Botha JF, Campos BD, Johanning J, Mercer D, Grant W, Langnas A. Endovascular closure of a hemiportocaval shunt after small-for-size adult-to-adult left lobe living donor liver transplantation. Liver Transpl 2009 Dec;15(12):1671-5
8. Yagi S, lida T, Taniguchi K, et al. Impact of portal venous pressure on regeneration and graft damage after living-donor liver transplantation. Liver Transpl 2005 Jan;11(1):68-75
9. Ogura Y, Hori T, El Moghazy WM, et al.Portal pressure <15 mm Hg is a key for successful adult living donor liver transplantation utilizing smaller grafts than before. Liver Transpl 2010 Jun;16(6):718-28
Citations
Citations to this article as recorded by