중심단어
mycotic aneurysm, iatrogenic injury, stent-graft
임상소견
후복막종양(extraskeletal osteosarcoma)을 주소로 내원 후 종양적출술을 시행받은 환자로 수술 도중 우측 외장골동맥과 우측 외장골정맥 손상이 발생하여 일차봉합술과 포가티 혈전제거술을 시행받음. 수술 후 지속적인 발열과 WBC (15.88 x 103/ul), CRP (9.81mg/dL) 상승이 있어 복부 전산화 단층촬영 (이하 복부 CT) 시행 후 복강 내 농양에 대해 경피적 배액술을 시행받음 (Fig. 1A). 당시 복부 CT에서 후복막종양 절제술 시행 부위와 우측 외장골동맥 주위에 염증소견이 관찰됨 (Fig. 1B). 경피적 배액술 시행 5시간 후 수축기 혈압이 60mmHg로 감소하고 헤모글로빈이 11.7g/dL에서 6.6g/dL로 감소하여 추가적인 복부 CT를 시행함.
진단명
Ruptured mycotic aneurysym at external iliac artery
영상소견
복부 CT에서 많은 양의 혈액이 복강외 공간 (extraperitoneal space)에 있고 우측 외장골동맥의 원위부에 진균성 동맥류가 있으며 이 부위에서 조영제의 혈관외 유출이 관찰됨 (Fig. 2).
시술방법 및 재료
우측 서혜부를 국소 마취한 후 초음파 유도 하에 21G micropuncture needle을 이용하여 우측 총대퇴동맥을 천자함. 5Fr micro-stick introducer sheath (Medcomp, Pennsylvania, USA)를 삽입한 후 조영제를 주입하여 동맥류의 위치를 확인함. 유도철사 (0.035” hydrophilic guidewire, Terumo, Tokyo, Japan)를 이용하여 조심스럽게 혈관손상 부위를 통과한 후 5Fr sheath (Terumo, Tokyo, Japan)를 삽입하여 시행한 우측 외장골동맥 혈관조영술에서 우측 외장골동맥의 원위부에 약 2.5cm 에 걸쳐 동맥류성 확장이 있고 전방외측에 거짓동맥류를 동반한 조영제의 혈관 외 유출이 있음을 확인함 (Fig. 3A). 이에 스텐트-그라프트를 삽입하여 거짓동맥류를 차단(exclusion)하기로 계획함. Proglide closure device 2개를 preclosing technique으로 걸어둔 후 5Fr sheath를 9Fr sheath (Terumo, Tokyo, Japan)로 교체하였음. 9mm x 5cm 스텐트-그라프트 (Viabahn, Gore, Arizona, USA)를 외장골동맥의 동맥류가 시작하는 부분에서 1.5cm 길이의 근위부 설치부위(proximal landing zone)를 확보하여 설치함 (Fig. 3B). 이후 시행한 우측 외장골동맥 혈관조영술에서 거짓동맥류가 더 이상 보이지 않고 조영제의 혈관외 유출이 소실됨을 확인함 (Fig. 3C). Proglide device를 사용하여 지혈함.
고찰
진균성 동맥류는 전체 동맥류의 0.8-2.8%를 차지할 정도로 드물지만, 파열되어서 혈복증를 일으키기 때문에 중요성을 간과할 수 없다. 본 증례에서 진균성 동맥류는 복강 내의 농양에 의한 패혈성 미세색전이 수술 도중에 후복막종양을 박리하면서 손상되었던 우측 외장골동맥에 도달하여 동맥벽을 감염시키고 약화시켜 동맥류를 형성하게 되었을 것으로 여겨진다. 그후 비교적 약한 부위인 일차봉합 부위가 파열되어 복막외강에 혈종이 발생하였다.
진균성 동맥류에서 스텐트-그라프트를 사용하는 것은 아직 논란의 여지가 있다. 여러 저자들은 수술 고위험환자에서 혈관 내 스텐트-그라프트가 감염성 동맥류의 일차적인 치료로 효과적이라고 하였으나 다른 저자들은 파열된 감염성 동맥류의 치료로 스텐트-그라프는 부적절하다고 하였다. 본 증례의 경우 외장골동맥의 동맥류가 파열된 환자로서 혈역학적으로 불안정하고 (수축기 혈압 60mmHg), 외장골동맥과 후복막종양과의 심한 유착으로 박리에 어려움이 있었던 경우로 외장골동맥류 파열에 대한 수술적 치료가 어려울 것으로 판단되어 응급으로 혈관내 치료를 시행하였다. 우측 총대퇴동맥 천자를 시작할 때부터 스텐트-그라프트가 설치될 때까지 소요된 시간은 30분 이내였고 시술 후 환자는 특별한 합병증을 보이지 않았으며 추적관찰에서 혈압과 헤모글로빈이 정상 수치를 보였다.
외장골동맥에서 발생한 동맥류가 파열되었을 경우 사망률은 30%에서 최대 50%에까지 이른다. 따라서 진균성 동맥류의 경우에도 본 증례의 경우처럼 혈역학적으로 불안정하고 수술적 치료가 어려운 경우 스텐트-그라프트를 이용한 치료가 장기적으로 문제를 일으킬 가능성은 있지만 life-saving procedure가 될 수 있다.
참고문헌
1. Richardson JW, Greenfield LJ. Natural history and management of iliac aneurysms. J Vasc Surg 1988;8:165-71.
2. Sandhu RS, Pipinos II. Isolated iliac artery aneurysms. Semin Vasc Surg 2005;18:209-15.
3. Stroumpouli E, Nssef A, Loosemore T, et al. The endovascular management of iliac artery aneurysm. Cardiovasc Intervent Radiol 2007;30(6):1099-1104.
4. Hecehlhammer L, Rancic Z, Pfiffner R, et al. Midterm outcome of endovascular repair of ruptured isolated iliac artery aneurysms. J Vasc Surg. 2010;52(5):1159 1163.
5. Rana MA, Kalra M, Oderich GS, et al. Outcomes of open and endovascular repair for ruptured and nonruptured internal iliac artery aneurysm. J Vasc Surg 2014;59(3):634-644
6. Polat KY, Aydini B, Keles M, et al. Spontaneous Mycotic External Iliac Artery Aneurysm Rupture after Perforated Acute Appendicitis in a Renal Allograft Recipient. Exp Clin Transplant. 2011;9(3):211-213.
7. Warren MJ, Fabian S, Tisi P. Endovascular PTFE covered stent for treatment of an external iliac artery pseudoaneurysm in the presence of chronic infection. Cardiovasc Intervent Radiol 2007;30(4):770-773.
8. Teodorescu VJ, Reiter BP. Common iliac artery pseudoaneurysm following inguinal hernia repair. Vasc Surg. 2001;35(3):239-244.
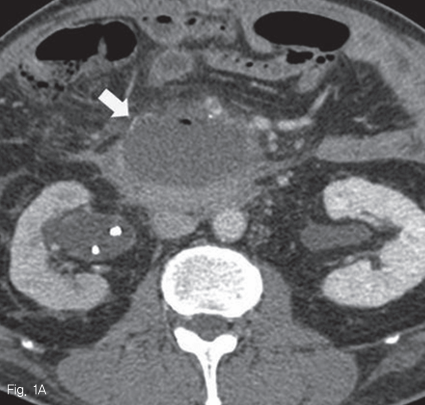
Fig 1A
The axial CT scan on portal phase shows a complicated fluid collection (arrow) in anterolateral aspect of 3rd portion of duodenum.
Fig 1B
The axial CT scan shows right external iliac artery (arrow) surrounding soft tissue attenuated inflammatory lesion (arrowhead).
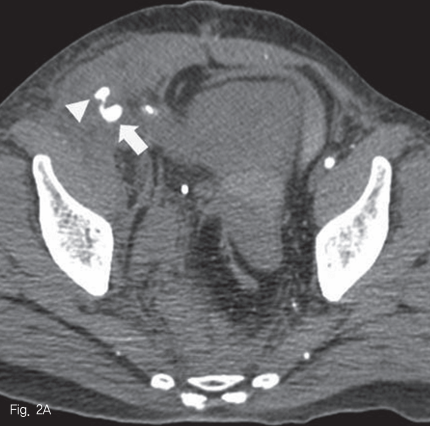
Fig 2A
The axial CT scan image on arterial phase shows aneurysmal dilatation of the right external iliac artery (arrow) with a surrounding inflammatory lesion/hematoma and extravasation of contrast material (arrowhead) from pseudoaneurysm.
Fig 2B
The axial CT scan image on portal phase shows several collections of contrast material (arrowhead) and large extra peritoneal hematomas (arrow).
Fig 2C
The volume rendering image shows segmental dilatation of right distal external iliac artery (arrow) with extravasation of contrast material (arrowheads).
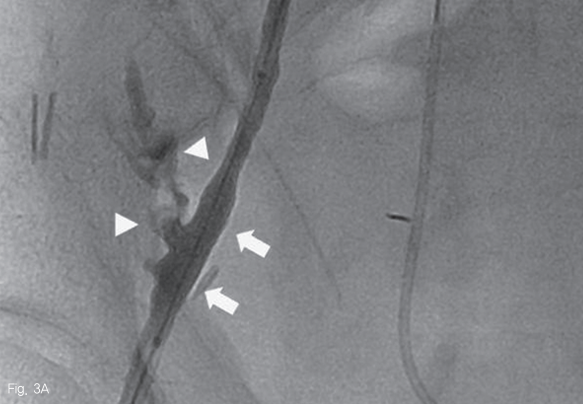
Fig 3A
Right external iliac artery angiogram shows mycotic aneurysm (arrow) at distal external iliac artery with extravasation of contrast material (arrowhead).
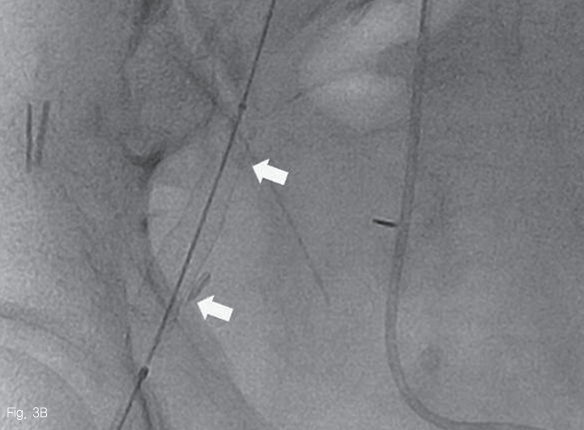
Fig 3B
A 9mm x 5cm stent-graft (arrow, Viabahn, Gore, Arizona, USA) was deployed in right distal external iliac artery for exclusion of pseudoaneurysm.
Fig 3C
On completion angiography, pseudoaneurysm is excluded and there is no visible extravasation of contrast material.
Citations
Citations to this article as recorded by