중심단어
Acute pancreatitis, pseudoaneurysm, embolization, superior mesenteric artery
임상소견
알코올 중독자로 하루 전날 과음을 한 후 우측 상복부 통증, 오심, 구토가 발생하여 내원하였다. 혈액 검사에서 Amylase/Lipase 수치가 110/94 U/L였다. 생체 징후는 혈압 150/90mmHg, 심박수 112회였으며 혈색소치는 13.7g/dl이었다.
진단명
Superior mesenteric artery pseudoaneurysm complicating acute pancreatitis
영상소견
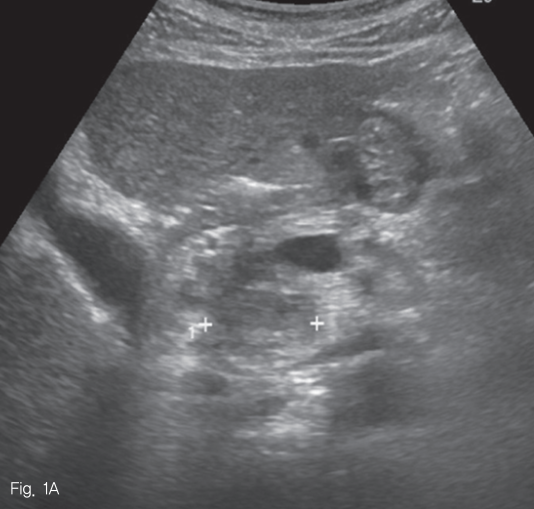
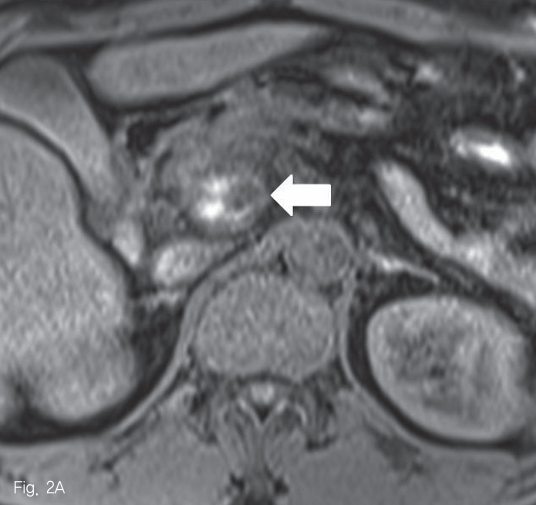
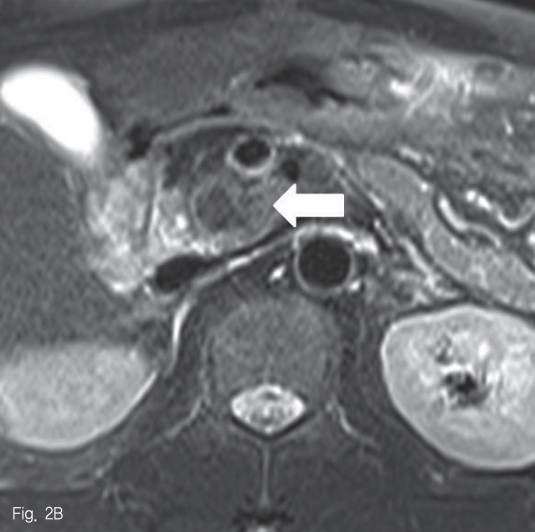
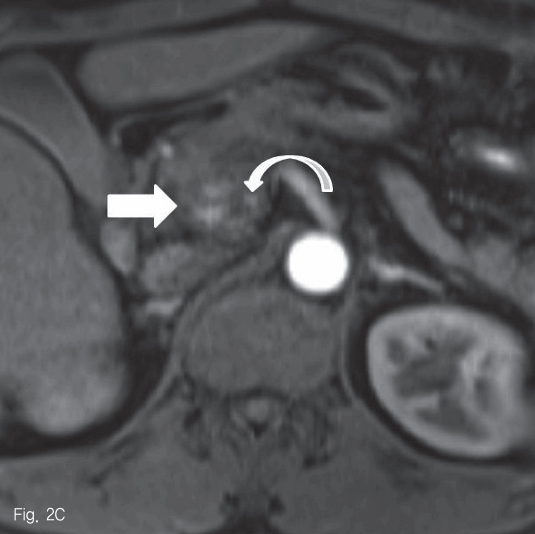
초음파 검사에서 췌장 두부에 약 2.5cm 크기의 종괴가 있었다 (Fig. 1). 췌장 자기공명영상에서 종괴는 T1-weighted image에서 다양한 신호강도를 보였고, T2-weighted image 에서는 저신호강도를 보여 다양한 단계의 출혈을 포함한 병변으로 생각하였다 (Fig. 2A-B). 조영 증강 자기공명영상 및 조영 증강 복부 전산화단층촬영에서 종괴의 내측으로 혈관과 비슷한 조영 증강을 보이는 1cm 크기의 병변이 보여 가성동맥류로 진단하였다 (Fig. 2C-D).
시술방법 및 재료
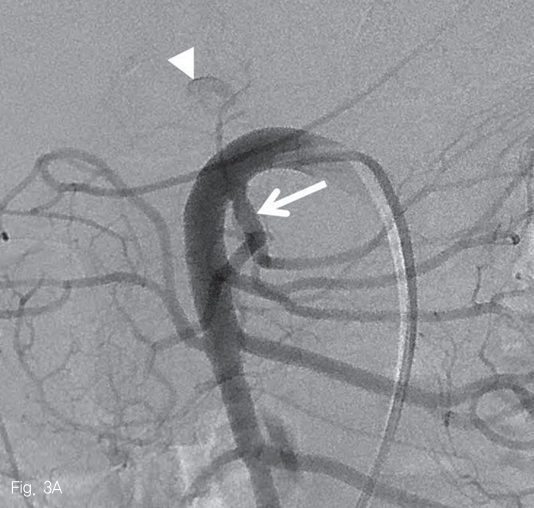
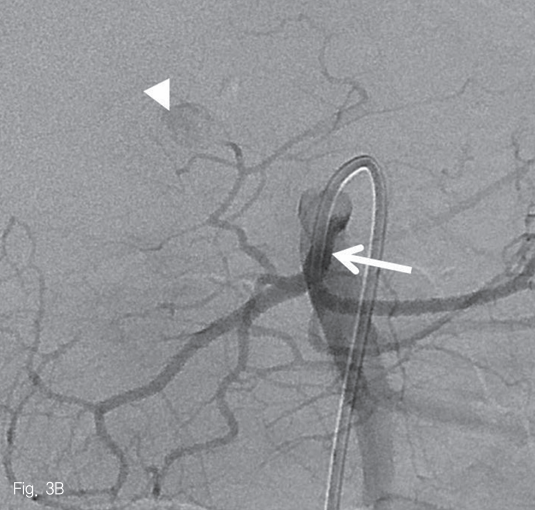
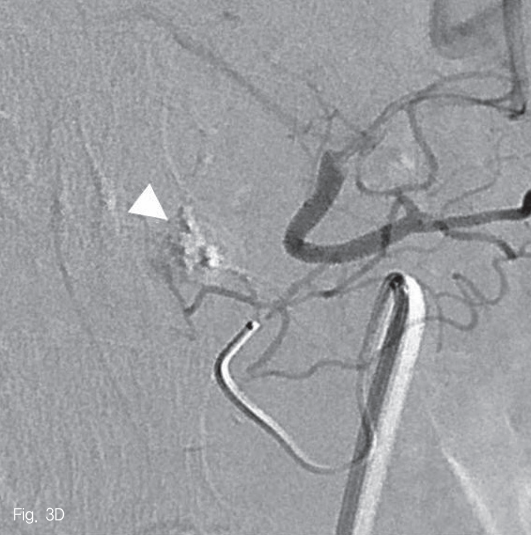
우측 대퇴동맥을 천자하여 5-Fr sheath(Radifocus; Terumo, Tokyo, Japan)를 삽입한 뒤, 5-Fr Cobra catheter(Cook Medical Inc, Bloomington, USA)를 사용하여 상장간막동맥 조영술을 시행하였다. 중간결장동맥의 근위부에 조영제가 채워지는 낭모양의 가성동맥류가 보였다 (Fig. 3A). 중간결장동맥은 상장간막동맥에서 후방으로 기시하여 5-Fr catheter로 선택하기 어려웠다. 0.035-in shapeable guidewire(Radifocus; Terumo, Tokyo, Japan)를 이용하여 중간결장동맥의 근위부까지 5-Fr catheter로 진입하였다 (Fig. 3B). 2.0-Fr microcatheter (Progreat; Terumo, Tokyo, Japan)를 이용해서 병변 직전까지 초선택하였다 (Fig. 3C). N-butyl-2-cyanoacrylate (Histocryl; B. Braun, Tuttlingen, Germany)과 Lipiodol (Guerbet, Paris, France)을 1:2 비율로 섞은 용액(33% glue)으로 색전술을 시행하였고 가성동맥류는 소실되었다 (Fig. 3D). 시술 직후 환자는 통증을 호소하였지만 곧 호전되었다.
추적관찰
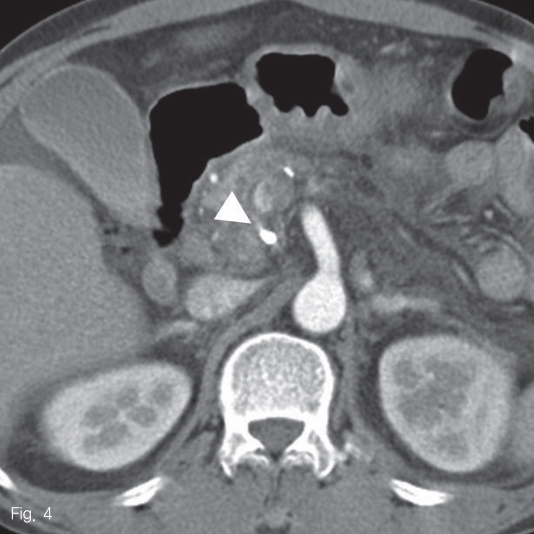
시술 후 혈청 amylase와 lipase 수치가 272U/L와 405U/L로 증가하였다가 3일 후에 정상화되었다. 시술 다음 날 시행한 조영 증강 복부 전산화 단층촬영에서 췌장의 가성동맥류에 glue로 인한 고음영 병변이 있었고 동맥류 내로 잔여 혈류는 보이지 않았다 (Fig. 4).
고찰
급성 췌장염은 염증이 진행함에 따라 주변 혈관을 침범하여 가성낭종 내에 출혈이나 혈전증, 정맥류, 가성동맥류 등을 유발할 수 있다. 췌장염으로 인한 가성동맥류는 췌장 효소로 인해 직접 혈관벽이 침식되어 발생하거나, 혈관 근처의 가성낭종 내의 췌장 효소에 의해 혈관벽이 침식되어 발생한다. 문헌에 의하면 췌장염으로 인한 가성 동맥류의 가장 흔한 위치는 비장동맥으로 30~50%를 차지하며, 위십이지장동맥은 10~15%, 췌십이지장동맥은 10%를 차지한다. 이 외에도 상장간막동맥, 간동맥, 복강동맥과 좌위동맥 등에서 발생할 수 있다고 알려져 있다.
가성동맥류가 발생한 환자들은 갑자기 심한 복통을 호소하거나 복부 팽만, 혈액 감소로 인한 심박수 증가, 저혈압 등을 주소로 내원한다. 일부 환자들은 혈변이나 흑색변을 주소로 내원하게 되나 급성 췌장염으로 인해 장기부전이 온 환자에서 위장관 출혈의 원인을 찾기는 어렵다. 가성동맥류를 진단하는데 있어서 혈관조영술이 가장 좋으나 항상 혈관조영술이 가능한 것이 아니므로 초기 진단에 CT를 이용한다. CT에서 가성낭종 내에 대동맥과 같은 정도로 조영증강이 되는 병변이 있으면 이를 가성동맥류로 진단을 할 수 있다. 급성 췌장염 환자 가운데 가성동맥류를 보이는 경우는 드물기는 하나 높은 사망률을 보이기 때문에 환자의 상태에 따라 조기 치료를 하는 것이 중요하다. 혈역학적으로 불안정한 환자의 췌장 가성동맥류는 수술로 치료하는 것이 좋으나 혈역학적으로 안정한 환자는 카테터를 이용한 색전술을 이용한다. 본 증례는 알코올 중독자에서 발생한 급성 췌장염의 가성동맥류로 내원 당시 환자는 혈역학적으로 안정한 상태였으므로 색전술을 시도하였다.
췌장염에서 출혈을 유발하는 혈관은 대부분이 작고 구불 구불한 경우가 많아서 직경이 큰 카테터를 이용해서 접근하는 것은 어렵다. 하지만, 본 증례에서처럼 미세카테터 만으로 가성동맥류까지 접근하는 것이 불가능할 수도 있다. 이런 경우 주요분지동맥을 5-Fr 카테터로 선택한 후에 미세카테터를 사용하는 것이 중요하다. 하지만, 중간결장동맥은 상장간막동맥의 후방에서 기시하는 경우가 많고 굴곡이 심해 5-Fr 카테터로 선택하기가 쉽지 않다. 본 증례는 0.035-in guidewire의 모양을 변형하여 중간결장동맥을 선택함으로써 병변의 색전술을 용이하게 할 수 있었다.
참고문헌
1. Mallick IH, Winslet MC. Vascular complications of pancreatitis. JOP 2004;5:328-337
2. Gleen W. Stambo MD, Michael J. Halliset MD, James J. Gallagher Jr. MD. Arteriographic embolization of visceral artery pseudoaneury. Annals of Vascular Surgery 1996;10:476-480
3. Mendelson RM, Anderson J, Marshall M, Ramsay D. Vascular complications of pancreatitis. ANZ J Surg 2005;75:1073-1079
4. Manase JR, Monzon JR, Dietz PA, Moglia R, Gold M. Treatment of pancreatic pseudoaneurysm with percutaneous transabdominal thrombin injection. J Vasc Surg 2003;38:600-602
5. S ftoiu A, Iordache S, Ciurea T, Dumitrescu D, Popescu M, Stoica Z. Pancreatic Pseudoaneurysm of the Superior Mesenteric Artery Complicated with Obstructive Jaundice: A Case Report. JOP 2005;6:29-35
Fig 1
Abdominal sonogram reveals a 2.5cm-sized mass in pancreatic head (cross signs).
Fig 2A
Pancreatic MRI reveals a mass in pancreatic head. It shows heterogeneous signal intensity in T1-weighted image (A, arrow) and low signal intensity in T2-weighted image (B, arrow).
Fig 2B
Pancreatic MRI reveals a mass in pancreatic head. It shows heterogeneous signal intensity in T1-weighted image (A, arrow) and low signal intensity in T2-weighted image (B, arrow).
Fig 2C
Contrast-enhanced MRI (C) and CT (D) images reveal well-enhancing nodular lesion (curved arrows) in medial aspect of the pancreatic mass (arrow).
Fig 2D
Contrast-enhanced MRI (C) and CT (D) images reveal well-enhancing nodular lesion (curved arrows) in medial aspect of the pancreatic mass (arrow).
Fig 3A
Arteriogram of superior mesenteric artery (SMA) shows a small pseudoaneurysm originating from the middle colic artery (A-C, arrowheads) which has large angle to backward (A). After the superselection of the bleeding branch (C), embolization with 33% glue was performed without any complication (D).
Fig 3B
Arteriogram of superior mesenteric artery (SMA) shows a small pseudoaneurysm originating from the middle colic artery (A-C, arrowheads) which has large angle to backward (A). After the superselection of the bleeding branch (C), embolization with 33% glue was performed without any complication (D).
Fig 3C
Arteriogram of superior mesenteric artery (SMA) shows a small pseudoaneurysm originating from the middle colic artery (A-C, arrowheads) which has large angle to backward (A). After the superselection of the bleeding branch (C), embolization with 33% glue was performed without any complication (D).
Fig 3D
Arteriogram of superior mesenteric artery (SMA) shows a small pseudoaneurysm originating from the middle colic artery (A-C, arrowheads) which has large angle to backward (A). After the superselection of the bleeding branch (C), embolization with 33% glue was performed without any complication (D).
Fig 4
An axial CT image shows hyperattenuated lesion by glue material within the previous pseudoaneurysmal sac without residual blood flow.
Citations
Citations to this article as recorded by