Introduction
Lipiodol을 이용한 ultra-selective TACE의 기본전략은 종양의 영양동맥을 통해 항암제를 섞은 Lipiodol을 천천히 주입하여 종양과 종양 주위의 문맥혈관까지 충분히 채운 후 gelfoam 등의 색전물질을 이용하여 영양동맥을 색전, 최종적으로 간동맥과 간문맥의 dual embolization을 유도하여 종양 및 종양주위를 괴사시켜 국소재발을 최소화시킨다라고 할 수 있다 (1). 이상적으로 종양을 완전히 괴사시키면서도 정상 간조직의 손상을 최소화하려면 microcatheter를 이용하여 종양의 가능한 모든 영양동맥을 ultra-selection해야겠으며, 이를 위해서는 종양의 영양동맥의 분지와 주행을 정확하게 파악하는 것이 선행되어야 한다. Flat panel detector와 cone-beam computed tomography(CBCT) 관련 기술이 발전하면서, 기존의 real-time fluoroscopy image, digital subtraction angiography (DSA) image 뿐만 아니라 MDCT처럼 transverse image 및 3D reconstruction image를 인터벤션실에서 환자의 이동 없이 혈관조영장비로 얻을 수 있게 되었고, 이를 TACE에 유용하게 사용하고 있다 (2-4). 이에 본 강의에서는 CBCT를 이용한 TACE의 이론적 내용을 간략히 설명한 후, 증례를 통해서 실제로 CBCT guided TACE를 시행할 때 도움이 될만한 세부적인 방법들에 대해 이야기하고자 한다.
CBCT hepatic arteriography - 3D navigation system for TACE
Table 1에서 MDCT와 CBCT를 서로 간략히 비교해보았다. CBCT의 flat panel은 주로 cesium iodide(CsI) fluorescence screen을 사용하는데, MDCT와 비교했을 때 detector efficiency가 좋지 않다 (5). 그래서, 같은 양의 전하를 이용하여 영상을 만들 때, contrast resolution이 떨어지고 noise 및 metallic artifact등에 취약하다. MDCT처럼 CBCT에서도 image reconstruction에 필요한 충분한 projection data를 얻기 위해서는 detector가 달려있는 C-arm이 180° + fan angle 정도 회전해야 하는데, 이에 약 6~10초정도 (vendor 및 model에 따라 다름)의 시간이 걸린다. 그러므로, MDCT보다 temporal resolution이 좋지 않아서 환자의 호흡, 움직임에 의한 motion artifact에 매우 취약하다. 이러한 약점들 때문에, 처음 CBCT 영상을 본 사람들은 이렇게 좋지 않은 영상으로 어떻게 TACE에 유용하게 쓰일 지 의문을 가질 수 있을 것이다. 반면에, CBCT는 MDCT와 비교했을 때 보다 작은 focal spot을 사용하고 보다 얇은 두께의 횡단영상을 얻을 수 있어서 MDCT보다 작은 크기의 voxel이 가능하고 보다 우월한 spatial resolution을 보여준다 (5). 이는 TACE를 시행하는데 있어 CBCT가 갖는 가장 큰 장점이다. Ultra-selective TACE를 시행하는데 있어 중요한 관심사는 조영 증강이 되는 종양과 조영제가 차있는 영양동맥이므로, CBCT의 우월한 spatial resolution은 보다 가는 영양동맥의 모습을 보여줄 수 있기 때문이다.
CBCT hepatic arteriography는 catheter를 시행하고자 하는 혈관에 위치시키고 조영제를 지속적으로 주입, C-arm이 돌아가면서 시행된다. 이렇게 얻은 projection data를 reconstruction하여 MDCT처럼 axial, coronal, sagittal을 포함한 2D MPR image와 volume rendering, MIP 등의 3D image를 얻을 수 있다. 특히, 조영제를 주입하는 catheter의 tip을 common hepatic artery나 proper hepatic artery에 위치시킨다면, 단 한 번의 시행으로 간동맥 전체 (물론, 해부학적 변이가 없는 경우에)의 CBCT hepatic arteriography를 얻을 수 있어, 종양의 유무, 종양의 위치, 종양의 영양동맥을 한 번에 평가할 수 있다. 또한, 최근의 장비는 3D image를 C-arm의 위치와 연동시켜 C-arm이 위치한 모든 방향의 3D image를 reference로 보여주어, 추가로 DSA를 시행하지 않고도 microcatheter를 영양동맥까지 진입하는데 있어 3D navigation 역할을 제공해준다. 최근의 연구결과에 따르면, 86명의 환자, 142개의 5cm 미만의 tumor에 대한 CBCT guided TACE를 분석했을 때, CBCT hepatic arteriography는 약 85%의 환자, 90%정도의 tumor에서 추가적인 혈관조영검사 없이 subsegmental TACE가 가능한 모습을 보여주었다 (6).
How can we obtain high quality images of CBCT hepatic arteriography?
CBCT hepatic arteriography를 이용하여 TACE를 성공적으로 시행하기 위해서 일단은 CBCT hepatic arteriography를 정확하게 시행하여 최대한 질 높은 영상을 얻는 것이 선행되어야 한다. 특히, 앞서 설명한대로 C-arm과 연동을 통한 3D navigation 역할을 위해서는 volume rendering 이나 MIP 등의 3D image가 매우 중요하다. 최근의 연구결과를 참조하여 CBCT hepatic arteriography에 영향을 주는 인자들에 이야기하도록 하겠다 (7).
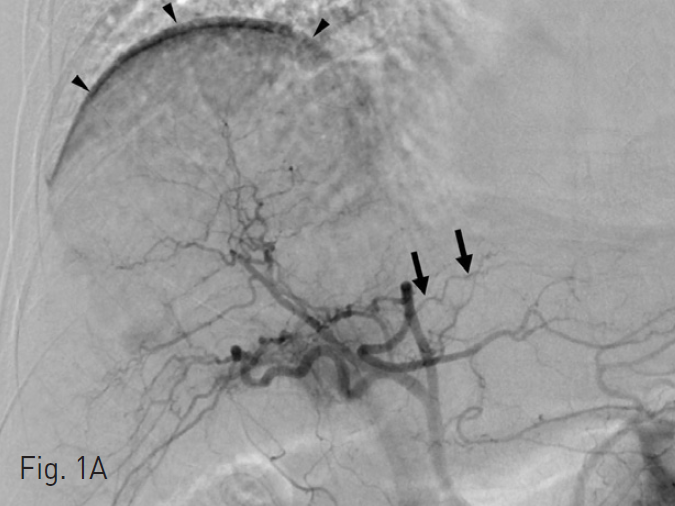
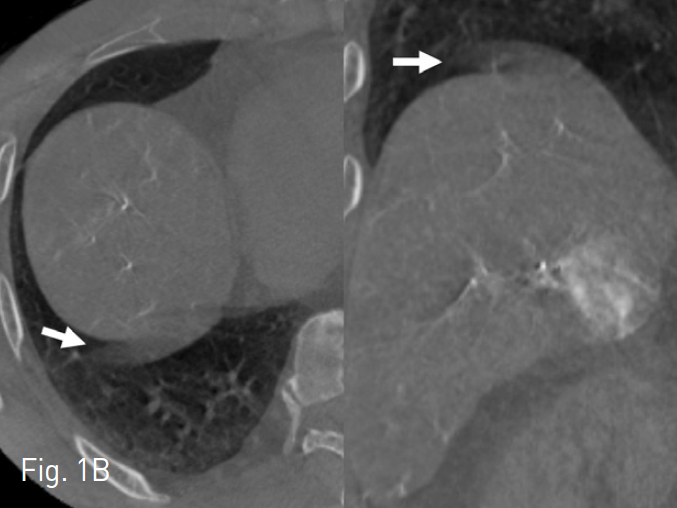
Detector의 크기가 고정되어 있고 C-arm이 제자리에서 회전 (MDCT의 spiral scan이 아닌 axial scan 처럼)하므로 결과적으로 MDCT와 비교했을 때 상당히 제한적인 FOV를 보인다. 참고문헌에 따르면, 체격이 상대적으로 작은 동양 환자임에도 불구하고 100명 중 29명의 환자에서 CBCT로 간 전체가 포함되지 않았다(7). CBCT 당시에 주로 right diaphragm dome쪽을 맞추고 시행되었기에 S2, S3, S6의 일부가 FOV에 포함되지 않는 일이 자주 발생했다. 앞서 설명한 대로, CBCT에서 C-arm이 회전하는데 약 6~10초의 시간이 걸리므로 temporal resolution이 좋지 않아서, 호흡조절이 제대로 협조되지 않는 환자의 경우 영상을 제대로 얻기가 불가능하다 (Fig. 1). 심지어 A2, A3의 경우 심장박동에 의한 움직임으로 인해 호흡 조절이 제대로 이루어 지더라도 motion artifact를 완전히 피하기가 어렵다 (Fig. 2).
Fig. 1. Motion artifact related to respiration
A. DSA image shows diaphragmatic motion artifact (arrowheads). However, A2(arrows) is definitely demonstrated.
B. Axial (right side) and coronal (left side) images show motion artifact of diaphragm (arrows).
C. Right oblique anterior view of CBCT MIP image shows severe blurring and discontinuity of right hepatic arteries (arrowheads). Even A2 is not visualized definitively (arrow).
Fig. 2
Motion artifact related to heart beat. CBCT MIP image with good breath-hold clearly shows fine branches of segmental arteries in the right hemiliver upto the subcapsular area. However, A2 and A3 show significant motion artifacts of blurring, double contour, and pruning of branches (arrowheads).
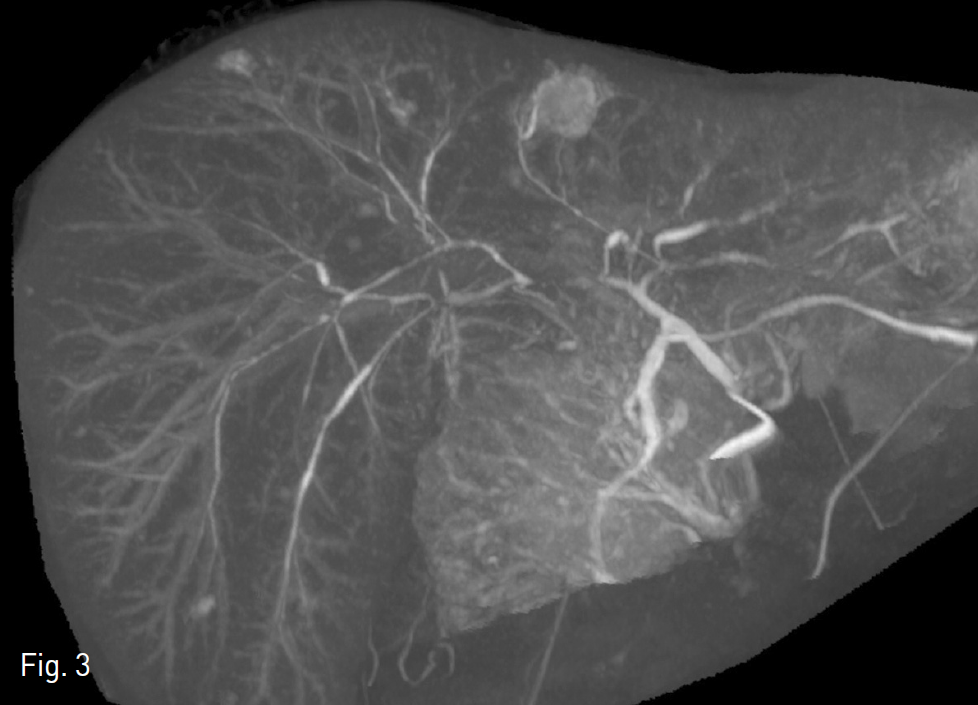
CBCT 시행할 때, 간동맥 이외 (splenic artery, gastroduodenal artery 등)로 주입된 조영제가 간문맥으로 들어오면서 CBCT 영상에 간문맥이 함께 보이는 경우 간동맥을 가리게 되어 영양동맥을 알아보는데 방해가 된다 (Fig. 3). 또한, 간동맥과 간실질 사이에 대조도 차이가 낮은 경우 가느다란 간동맥들이 보이지 않아 영양동맥을 알아보기 힘들게 된다 (Fig. 4). 이 같은 모습들은 환자의 혈류속도, 혈류량, catheter tip의 위치, X-ray delay 등에 영향을 받는다. 생리식염수를 통해 희석한 조영제를 사용하여 CBCT를 시행한다면, 2D image에서 beam hardening artifact를 줄일 수가 있겠지만, 간동맥과 간실질과 의 대조도를 떨어뜨려 3D image에서 가느다란 간동맥을 보여주는 것이 어려워진다.
Fig. 3
Significant portal vein enhancement. Right portal vein branches are visualized upto the subcapsular area, which disturbs the tracing of the hepatic artery.
Fig. 4
Low hepatic artery-to-parenchyma enhancement ratio. There is abrupt tapering of multiple hepatic arteries(arrowheads) without demonstration of fine branches around the subcapsular area on CBCT MIP images.
이러한 내용을 바탕으로 저자가 CBCT를 시행하는 방법을 간략히 소개하고자 한다. 5 Fr RH catheter 또는 2.7 Fr microcatheter를 이용하여 CBCT를 시행하고자 하는 위치에 catheter의 tip을 위치시킨다. Proper hepatic artery가 이상적이겠지만, vasospasm이 일어나기 쉽고 해부학적으로 proper hepatic artery가 짧거나 없는 경우가 많으므로 common hepatic artery가 제일 흔히 시행된다. 일단은 DSA를 시행하여 간동맥의 혈류속도, 종양의 위치를 대략적으로 확인한다. 종양이 CBCT의 FOV에 벗어나지 않도록 주의하면서 환자 table의 위치를 설정한다. 조영제의 양, X-ray delay는 앞서 시행한 DSA를 보면서 설정한다. Splenic artery 쪽으로 많은 조영제가 역류되지 않으면서도 common hepatic artery를 충분히 채울 정도의 조영제 속도로 주입하며, 조영제가 간의 변연부에 도달할 때 CBCT scan이 시작되도록 X-ray delay를 설정한다. 경험적으로 common hepatic artery 에서는 2.5~3.5ml/s의 속도로 3~5초 X-ray delay가 대부분 사용된다. 물론 이 모든 것보다 가장 중요한 것은 호흡조절에 대한 환자의 협조이므로 CBCT 시행 전 환자에게 충분한 설명과 연습을 시행해야 하겠다.
맺음말
지금까지 CBCT hepatic arteriography에 대한 이론적인 내용에 대해 간략히 설명하였다. 좀 더 실질적인 이해와 도움이 되고자, 본원에서 시행한 55세 남자환자의 CBCT guided TACE case를 처음부터 끝까지 동영상 위주로 review하면서 실제로 CBCT guided TACE를 시행할 때 세부적인 방법들에 대해 이야기하고 강의를 마치고자 한다.
참고문헌
1. Miyayama S, Matsui O, Yamashiro M, et al. Ultraselective transcatheter arterial chemoembolization with a 2-f tip microcatheter for small hepatocellular carcinomas: relationship between local tumor recurrence and visualization of the portal vein with iodized oil. J Vasc Interv Radiol 2007;18(3):365-376.
2. Kakeda S, Korogi Y, Ohnari N, et al. Usefulness of cone-beam volume CT with flat panel detectors in conjunction with catheter angiography for transcatheter arterial embolization. J Vasc Interv Radiol 2007;18(12):1508-1516.
3. Tognolini A, Louie JD, Hwang GL, Hofmann LV, Sze DY, Kothary N. Utility of C-arm CT in patients with hepatocellular carcinoma undergoing transhepatic arterial chemoembolization. J Vasc Interv Radiol 2010;21(3):339-347.
4. Wallace MJ, Murthy R, Kamat PP, et al. Impact of C-arm CT on hepatic arterial interventions for hepatic malignancies. J Vasc Interv Radiol 2007;18(12):1500-1507.
5. Kalender WA, Kyriakou Y. Flat-detector computed tomography (FD-CT). Eur Radiol 2007;17(11):2767-2779.
6. Lee IJ, Chung JW, Yin YH, et al. Cone-Beam Computed Tomography (CBCT) Hepatic Arteriography in Chemoembolization for Hepatocellular Carcinoma: Performance Depicting Tumors and Tumor Feeders.Cardiovasc Intervent Radiol 2015 [Epub ahead of print].
7. Lee IJ, Chung JW, Yin YH, et al. Cone-beam CT hepatic arteriography in chemoembolization for hepatocellular carcinoma: angiographic image quality and its determining factors. J Vasc Interv Radiol 2014;25(9):1369-1379.
Citations
Citations to this article as recorded by