중심단어
Solitaire, secondary hypertension, renal artery, percutaneous angioplasty
임상소견
Cerebral palsy와 developmental delay의 기왕력이 있고 나이에 비해 신체발달이 느림. 고혈압을 주소로 내원 후 시행한 복부 CT에서 우측 신장동맥에 협착증이 발견되어 이차성 고혈압으로 진단됨. 우측 신장동맥 협착증의 치료를 위해 우측 신장동맥의 percutaneous angioplasty (PTA) 의뢰됨. 시술 도중 신장동맥 분지에 색전물질에 의한 폐쇄가 발생하여 aspiration을 수 차례 시행하였으나 실패하여 Solitaire FR revascularization device를 사용하여 emboli를 제거함.
진단명
Embolic occlusion of right renal artery after percutaneous angio plasty
영상소견
복부 CT에서 대동맥에 diffuse narrowing이 있고 우측 신장동맥에 severe stenosis가 있음 (Fig. 1A).
시술방법 및 재료
우측 서혜부를 국소 마취한 후 초음파 유도 하에 21G micropuncture needle (Cook medical, Bjaeverskov, Denmark)을 이용하여 우측 총대퇴동맥을 천자함. 4Fr sheath (Terumo, Tokyo, Japan)를 삽입 후 4Fr pigtail catheter를 이용하여 시행한 복부대동맥 조영술에서 대동맥의 diffuse narrowing이 있고 우측 신장동맥의 중간부위에 severe stenosis가 있음을 확인함 (Fig. 1B). 혈전생성을 막기 위해 ⅣV를 통해 heparin 3000IU를 주입함.
4Fr cobra catheter (Terumo, Tokyo, Japan)를 우측 신장동맥의 입구에 위치시킨 후 microferret microca theter (Cook medical, Bjaeverskov, Denmark)와 meister microwire (ASAHI, Aichi, Japan)를 이용하여 조심스럽게 ste no tic portion을 지나간 후 SV-5를 삽입하여 그 끝을 우측 신장동맥의 원위부에 위치시킴. Microcatheter와 4Fr cobra catheter를 제거한 뒤 2mm x 2cm balloon catheter를 이용하여 PTA 시행함. Follow up angiography에서 50% 이상의 stenosis가 남아 있어 3mm x 2cm balloon catheter를 이용하여 PTA 시행함 (Fig. 2). Follow up angiography에서 right renal artery의 midportion에 dissection이 발생함을 확인하여 2mm x 2cm balloon catheter를 3mmHg까지 inflation하여 balloon tamponade를 3분간 시행함 (Fig. 3). Follow up angiography에서 dissection은 호전되었으나 anterior divisional artery와 posterior divisional artery가 emboli에 의해 막힘 (Fig. 4). Microferret catheter를 이용하여 aspiration thrombectomy를 수 차례 시행하였으나 여전히 남아있음.
Solitaire FR (COVIDIEN, CA, USA, Fig.5)을 이용하여 mechanical thrombectomy를 계획하고 4Fr cobra catheter를 right renal artery 입구에 위치시킨 후 Excelsior XT-27 (Striker, CA, USA)를 occlusive lesion을 통과하여 삽입 후 Solitaire FR stent를 emboli에 의해 막힌 부위를 충분히 cover하여 deployment 시킴. 5분 뒤 조심스럽게 Solitaire FR stent를 당겨서 mechanical thrombectomy를 시행함. 신장동맥 anterior division의 emboli는 성공적으로 제거되었으나 시술 당시에 posterior division이 막힌 것을 파악하지 못하고 anterior division의 embolic material만 제거한 상태에서 시술을 종료함 (Fig. 6A,B).
Fig. 1
A-B. The volume rendering image and aortogram show severe stenosis of mid portion of right renal artery and diffuse narrowing of abdominal aorta.
Fig. 2
Balloon angioplasty was done at severe stenosis of right renal artery with 2mm x 2cm balloon catheter and 3mm x 2cm balloon catheter.
Fig. 3
After balloon angioplasty, dissection was developed at right renal artery.
Fig. 4
Right renal artery angiogram shows distal occlusion of right renal artery.
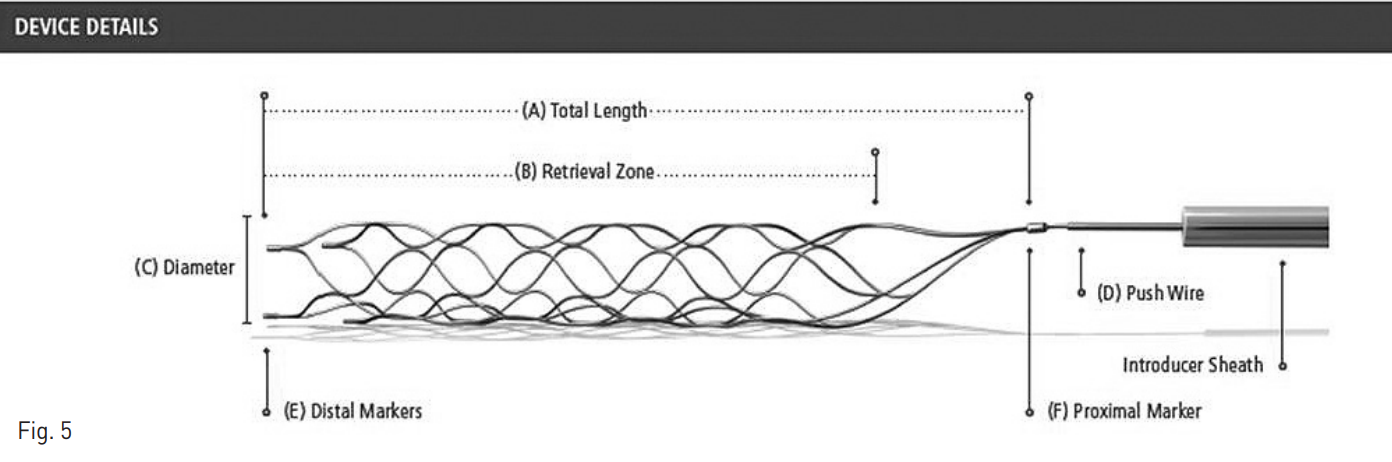
Fig. 5
Schematic image shows Solitaire FR revascularization device.
Fig. 6
A. After mechanical thrombectomy with Solitaire FR, right renal angiogram shows patent anterior divisional branch of right renal artery.
B. Photo image shows embolic material with Solitaire FR.
고찰
신장동맥 협착증은 신장혈류를 감소시킴으로 인해 심각한 이차성 고혈압, 신장기능 부전, 말기신부전을 일으키는 원인이 된다. Percutaneous angioplasty 또는 수술적 치료가 신장의 관류를 개선시키는데 이용되는데 현재는 percutaneous angioplasty가 우선적인 치료로 이용된다. 그러나 좁아진 혈관을 풍선을 이용하여 확장시키는데 있어서 embolism에 의한 신장동맥분지의 폐쇄가 보고가 되어 왔고 Edwards et al.에 의하면 풍선 확장술에 의해 발생되는 emboli는 약 2000개가 넘는다고 하였다. 대부분의 emboli는 크기가 작아 시술도중에 발견이 어렵고 대부분은 증상이 없지만 일부의 경우 큰 emboli에 의해 말단신장동맥의 폐쇄가 발생할 수 있고 이 부위의 신장관류 저하를 야기할 수 있다.
Emboli에 의한 혈관의 폐쇄를 치료하는 경우 카테터를 이용한 aspiration을 시행하거나 primary stenting을 시행하게 된다. 그러나 혈관의 크기가 작은 경우는 스텐트 삽입술을 시행하기 어렵고 aspiration을 시행하더라도 내경이 작은 카테터 또는
microcatheter를 사용할 수 밖에 없어 성공률이 낮아지게 된다.
Solitaire FR revascularization device는 두개내혈관 폐색으로 인한 허혈성 뇌졸중 환자의 혈류 복원을 위해 사용되며, 정맥 조직 플라스미노겐 활성제 (IV tPA)에 부적합하거나 해당 요법에 실패했던 환자들을 대상으로 사용하게 되어 있어 말초혈관을 대상으로 한 시술은 의료보험 적용을 받을 수는 없다. 그러나 본 증례의 경우처럼 혈관 내경이 작아 microcatheter를 이용하여 aspiration을 시도하였으나 실패하고 스텐트 삽입술이 어려운 경우, Solitaire FR revascularization device를 이용한 mechanical thrombectomy는 또 다른 치료대안이 될 수 있다.
참고문헌
1. Edwards MS, Corriere MA, Craven TE, et al. Atheroembolism during percutaneous renal artery revascularization. J Vasc Surg. 2007 Jil;46(1):56-61.
2. Edwards MS, Craven TE, Burke GL, et al. Renovascular disease and the risk of adverse coronary events in the elderly ? a prospective, population-based study. Arch Internal Med 2005;165:207-13.
3. Fried LF, Shlipak MG, Crump C, et al. Renal insufficiency as a predictor of cardiovascular outcomes and mortality in elderly individuals. J Am Coll Cardiol 2003;41:1364-72.
4. Johansson M, Herlitz H, Jensen G, et al. Increased cardiovascular mortality in hypertensive patients with renal artery stenosis. Relation to sympathetic activation, renal function, and treatment regimens. J Hypertens 1999;17:1743-50.
5. Baumgartner I, von Aesch K, Do DD, et al. Stent placement in ostial and nonostial atherosclerotic renal arterial stenoses: a prospective follow-up study. Radiology 2000;216:498-505.
6. Lederman RJ, Mendelsohn FO, Santos R, et al. Primary renal artery stenting: characteristics and outcomes after 363 procedures. Am Heart J 2001;142:314-23.
7. Tuttle KR, Chouinard RF, Webber JT, et al. Treatment of atherosclerotic ostial renal artery stenosis with the intravascular stent. Am J Kidney Dis 1998;32:611-22.
Citations
Citations to this article as recorded by