중심단어
Axillofemoral, bypass graft occlusion, mechanical thrombectomy, angioplasty
임상소견
Aorto-iliac occlusive disease (Leriche's syndrome)로 9년 전 우측 액와-대퇴 우회술 및 대퇴-대퇴 우회술 시행 받았음 (Fig. 1). 3개월 전 시행한 Lower extremity CT angiography에서는 우회로의 patency가 잘 유지되어 있었으나 일주일 전부터 양측 하지의 차가운 느낌이 발생하였고 1일 전부터 양측 하지의 통증이 발생하여 내원함. 우측 슬와동맥과 족배동맥은 매우 약하게 촉지되었으며 좌측 슬와동맥과 족배동맥은 거의 촉지되지 않았음.
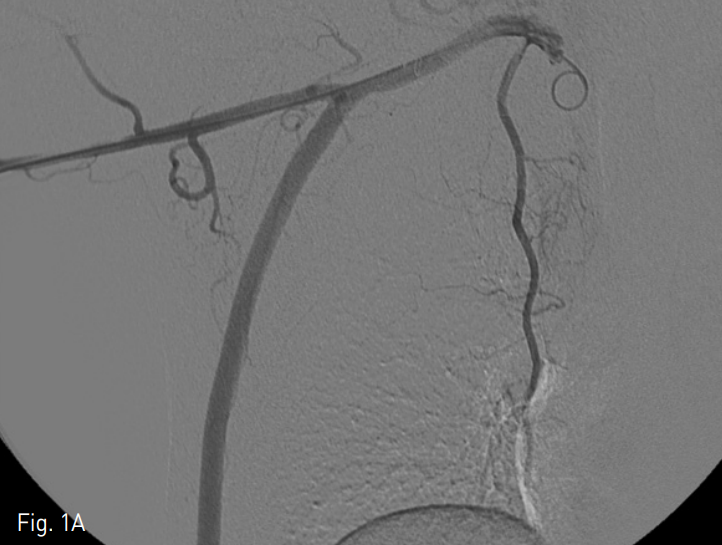
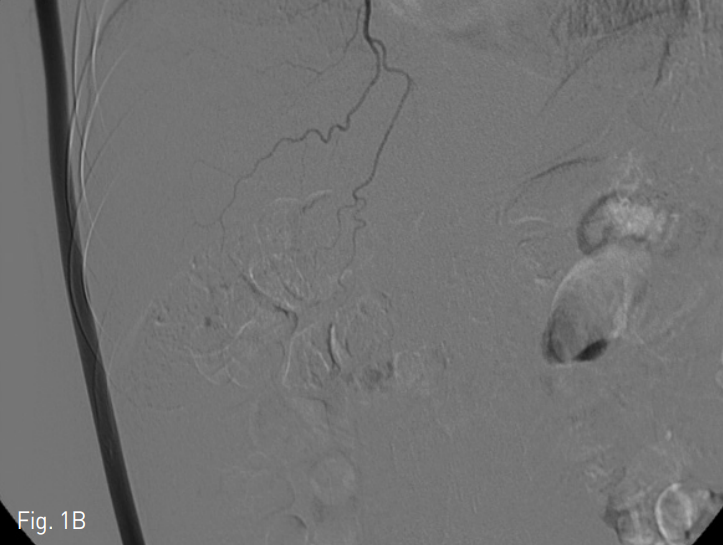
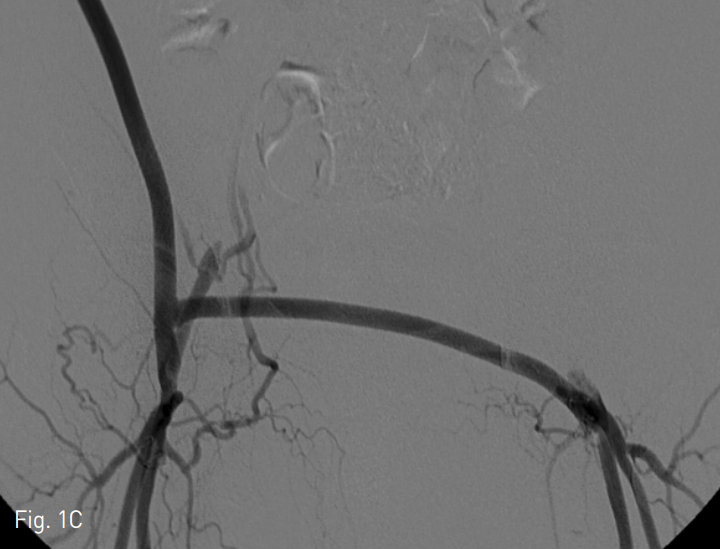
Fig. 1
A-C. Arteriogram obtained from the right subclavian artery shows patent blood flow through the right axillofemoral bypass and femorofemor al bypass grafts without stenosis.
진단명
Thrombotic occlusion of axillofemoral bypass and femorofemoral bypass grafts
영상소견
전산화 단층촬영에서 우측 액와-대퇴 및 대퇴-대퇴 우회로의 혈전성 완전폐쇄가 관찰되었으며 액와-대퇴 우회로 문합부의 협착이 동반되어 있었다 (Fig. 2). 우회로보다 원위부에 위치한 표재대퇴동맥, 슬와동맥 및 무릎 아래 동맥들의 혈류는 collateral을 통하여 유지되어 있었다.
시술방법 및 재료
액와-대퇴 우회로의 중간부, 원위부와 대퇴-대퇴 우회로의 근위부를 천자하여 각각 8Fr sheath (Terumo, Tokyo, Japan)를 삽입한 후 총 3개의 access site를 이용하여 thrombus의 mechanical aspiration을 시행하였다. Aspiration을 통해 우회로 내부 대부분의 thrombus는 제거되었고 우측 액와동맥-우회로 문합부의 arterial plug에 대해서는 Fogarty balloon catheter (Applied Medical, Rancho Santa Margarita, CA, USA)를 이용하여 제거하였다. 대퇴-대퇴 우회로 내부에 관찰되는 chronic adherent thrombus에 대해서는 7mm balloon catheter (Mustang, Boston Scientific Corporation, Natick, MA, USA)를 이용하여 angio plasty를 시행하였다. 우측 액와동맥-우회로 문합부와 양측 총대퇴동맥-우회로 문합부에 협착이 관찰되어 5mm, 6mm balloon catheter(Mustang, Boston Scientific Corporation, Natick, MA, USA)를 이용하여 angioplasty를 시행하였다. 이후 양측 총대퇴동맥-우회로 문합부에 관찰되는 elastic recoil에 대하여 5mm cutting balloon catheter (Boston Scientific Corporation, Natick, MA, USA)로 cutting balloon angioplasty를 시행하였으나 지속적으로 flow limitation이 관찰되어 각각 6mm/4cm bare metallic stent (Complete SE, Medtronic, Minneapolis, MN, USA)를 이용한 bail-out stenting을 시행하였다. 시술 후 시행한 조영술에서 액와-대퇴 및 대퇴-대퇴 우회로의 혈류가 회복된 것을 확인할 수 있었다 (Fig. 3). 3개의 access sites에 대하여 FemoSeal® vascular closure system (St. Jude Medical, Uppsala, Sweden)을 사용하였고 성공적으로 지혈되었다.
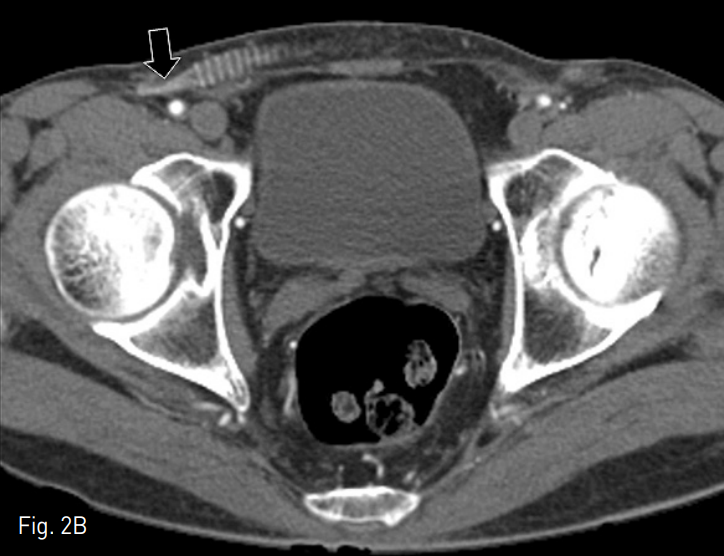
Fig. 2
A-B. Contrast-enhanced coronal CT shows completely occluded bypass grafts (white arrows) and collapsed anastomotic sites at distal portion of right axillofemoral graft and proximal portion of femorofemoral graft (black arrows).
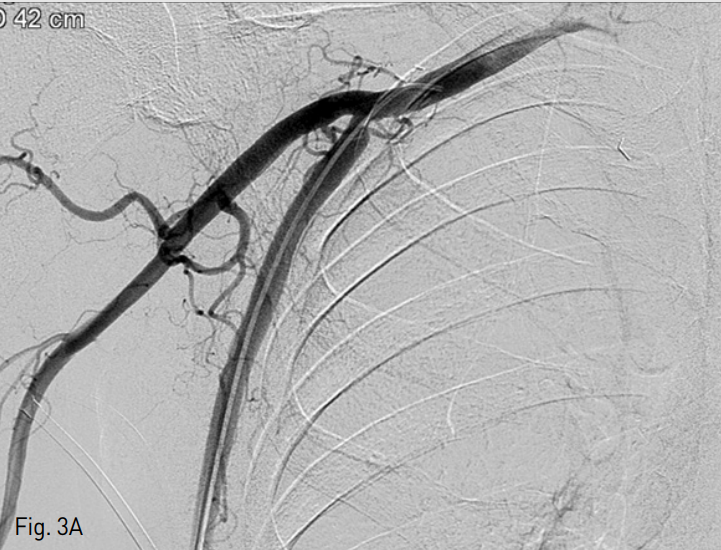
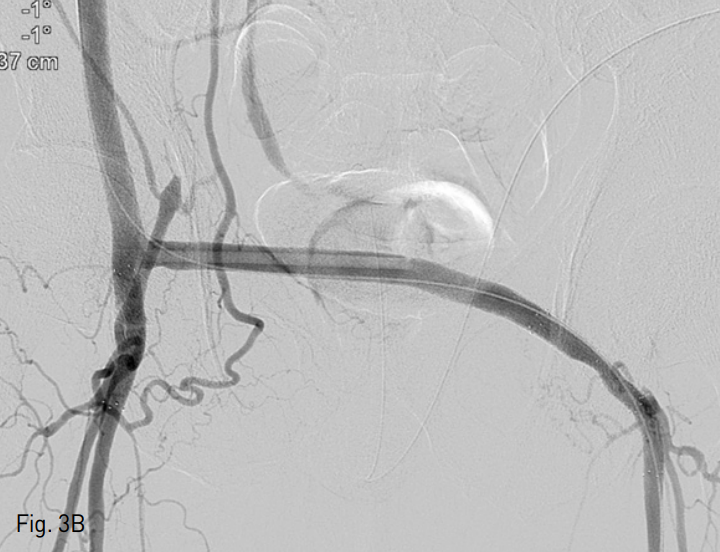
Fig. 3. Arteriogram obtained from catheter inside bypass graft shows restored patency of axillofemoral and femorofemoral bypass grafts.
A. Restored blood flow in the right axillary artery and bypass graft.
B. Bare metallic stents inserted at anastomosis sites between both common femoral arteries and bypass grafts, with improved stenosis.
추적관찰
시술 후 1개월 간격으로 외래 진료를 통한 추적 관찰을 하였고 주관적인 증상은 호전되었으며 3개월 후까지 좌우 하지의 혈관 박동이 잘 촉지됨을 확인할 수 있었다.
고찰
액와동맥은 대동맥-양측 대퇴 우회술을 받기에 적합하지 않은 환자들에게 있어서 대안적인 inflow source로 많이 사용되며, 액와-대퇴 우회술을 받는 대상군들은 대체적으로 대동맥-대퇴 우회술을 받는 환자들에 비해서 나이가 많고 시술에 대한 사망률의 위험도가 증가되어 있으며 더 짧은 예측수명을 가지는 특징을 보인다. 액와-대퇴 우회로의 폐쇄는 근위부 또는 원위부 anastomosis 부분의 stenosis, graft의 kinking 등의 선행인자에 따른 혈전의 생성에 의해 발생하며 일부에서는 arterial occlusive disease가 우회로까지 progression함으로써 발생한다. 이러한 bypass graft의 혈전성 폐쇄에 대해서는 수술적인 방법을 통한 혈전 제거 및 graft revision이 gold standard로 여거져 왔지만 액와-대퇴 우회술을 받게 되는 환자들의 기본적인 특징과 second operation에 따른 높은 위험률, 그리고 신경의 손상, 출혈, 긴 수술 시간과 입원 기간에 따른 위험도와 같은 수술적인 방법에 동반될 수 있는 complication들을 고려하면 수술적 방법들은 제한적일 수 있다. 또한, 혈전 제거술에 더불어서 애초에 혈전을 발생시키게 되는 선행요인을 수술적으로 해결하기 위해서는 graft를 아예 take down하고 새로 interposition해야 된다는 점도 수술적인 방법의 제한점으로 작용한다.
따라서 이런 제한점을 회피하기 위한 경피적 혈관 내 접근을 통한 중재술을 사용한 증례들이 보고되었는데, 주된 방법으로는 상완동맥의 천자 후 catheter를 통한 thrombectomy와 overnight thrombolysis가 사용되었으며 추가적으로 anastomosis부분에 stenosis가 있는 경우에는 angioplasty와 필요 시 stent placement가 시행되었다. Recanalization은 대부분 성공적이었으며, 한 보고에서는 2 year primary pa tency가 58% 까지 보고되었다.
본 증례에서는 bypass graft의 direct puncture를 통하여 시술을 하였고 이로 인해 상완동맥의 천자에 따를 수 있는 complication을 피할 수 있었다. 또한 상완동맥의 천자를 통하여 시술하는 것에 비해 보다 큰 Fr의 sheath (8Fr)를 사용하여 직경이 큰 액와-대퇴 우회로의 내부에 존재하는 많은 양의 혈전을 모두 제거할 수 있었고, overnight thrombolysis 없이 single session으로 시술을 종료하여 thrombolysis에 따를 수 있는 출혈의 risk를 감소시킬 수 있었다. 본 증례에서 anastomotic site의 site의 stenosis에 대하여 balloon angioplasty를 시행한 후 elastic recoil에 의한 flow limitation이 지속적으로 관찰되었는데, 이는 stenosis가 atherosclerotic lesion이라기 보다는 수술 후 변화에 의한 fibrotic lesion이기 때문에 관찰되는 현상이라고 생각되었으며, 이의 해결을 위해 bail-out stenting을 시행하였다. 환자가 우회술을 받은 시기는 9년 전으로 pseudoendothelium이 형성되었을 것이라고 생각되었고 시술 후 closure device를 이용하여 bleeding 없이 세 군데 모두 성공적으로 sealing 되었다.
참고문헌
1. Wayangankar S, Patel J, Hennebry TA. Isolated pharmaco-mechanical thrombectomy (IPMT) for the endovascular treatment of acute axillofemoral graft occlusion. Vasc Med. 2013;18:27-31.
2. Eisenberg JA, Calligaro KD, Kolakowski S et al. Is balloon angioplasty of peri-anastomotic stenoses of failing peripheral arterial bypasses worthwhile? Vasc Endovascular Surg. 2009;43:346-351.
3. Slovut DP, Bacharach JM. Endovascular treatment of an occluded axillofemoral bypass graft. Vasc Med. 2005;10:33-36.
4. Olson CJ, Edwards JM, Taylor LM, Landry GJ, Yeager RA, Moneta GL. Repeat axillofemoral grafting as treatment for axillofemoral graft occlusion. Arch Surg. 2002;137:1364-1367; discussion 1367-1368.
Citations
Citations to this article as recorded by