중심단어
Vertebral artery pseudoaneurysm, central venous catheter, internal jugular vein, coil embolization
임상소견
60세 남자가 점차 심해지는 폐부종과 폐렴, 전신쇠약감을 주소로 내원하였다. 환자는 당뇨, 고혈압, 만성 신부전의 병력이 있다. 환자는 병동에서 응급 투석을 위하여 우측 내경정맥을 통하여 중심정맥관 삽관을 시도하였다. 시술은 내과 1년차 전공의가 실시하였으며 시술도중 유도철사를 통해 8 Fr 확장관을 넣었다 뺀 이후 시술부위에서 동맥피가 솟구쳐 올라서 시술 도구들을 모두 제거한 뒤 손으로 압박을 실시하였으나 환자는 수축기 혈압이 50까지 떨어지면서 의식상태가 저하되어 응급 심폐소생술이 실시 되었다. 이때 우측 쇄골하정맥관이 추가로 삽입되었다.
진단명
A large vertebral artery pseudoa neurysm due to percutaneous internal jugular vein cannulation
영상소견
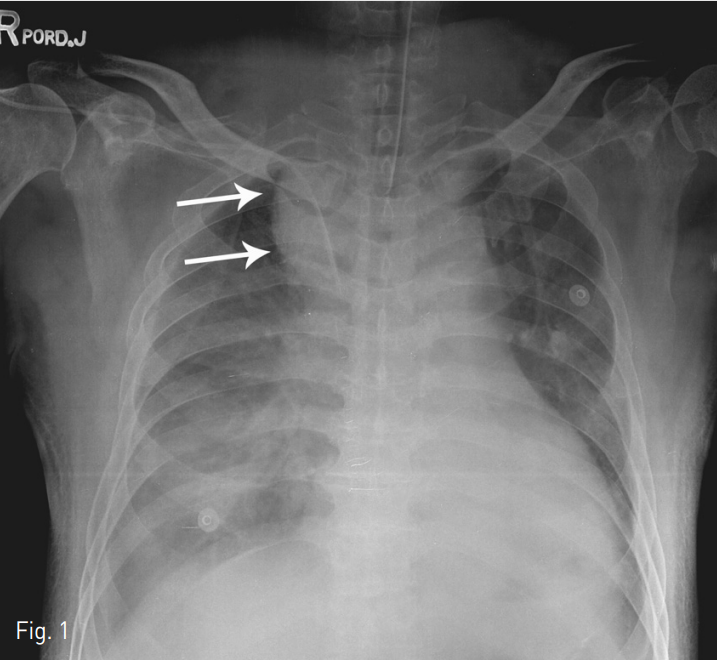
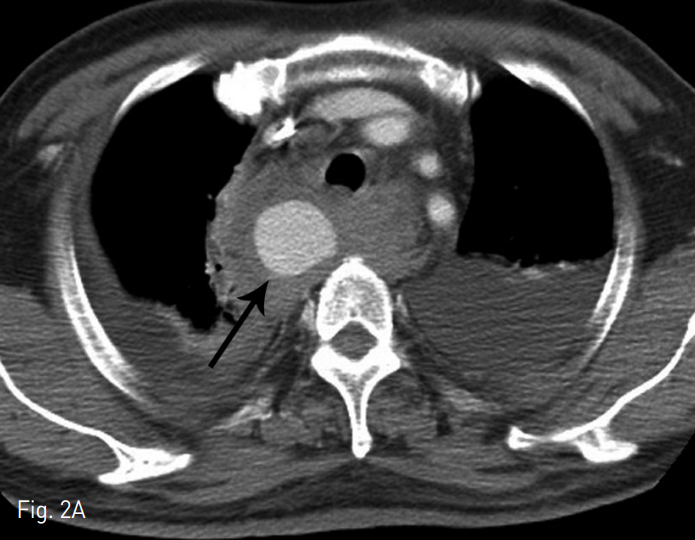
단순 X-ray촬영상 기관지 우측으로 확장된 음영이 관찰되었고 (Fig. 1) CT 검사상 우측 척추동맥에서 발생된 큰 가성동맥류가 관찰되고 (Fig. 2) 우측 종격동내에는 다량의 혈종이 보였다.
Fig. 1
Plain chest x-ray showing the bulging contour of right paratracheal area (arrows) and supra-mediastinal widening.
Fig. 2
Axial (A) and multiplanar reformatted (B) images showing large pseudoaneurysm (black arrows) at the right side supramediastinum with surrounding hematoma. The pseudoaneurysm is originated from proximal right vertebral artery (VA, white arrow)
시술방법 및 재료
환자는 인터벤션 시술실에서 응급 혈관조영술을 실시하였고 우측 쇄골하정맥 직상부 우측 척추동맥에서 발생한 큰 가성동맥류가 확인되었다. 또한, 좌측 척추 동맥이 잘 유지된 것을 확인하였다. 4 Fr 혈관촬영용 도관 (JB2, Cook, Inc .; Bloomington, IN, USA)을 척추동맥으로 넣은 후 가성동맥류 원위부부터 두 개의 5mm, 한 개의 4mm 금속코일 (Nester, Cook)로 척추동맥을 색전한 후 10mm x 25mm 풍선확장형 스텐트 그라프트 (Jomed International AB, Helsingborg, Sweden)을 척추동맥 기시부에 걸쳐서 우측 쇄골하 정맥에 위치시켰다.
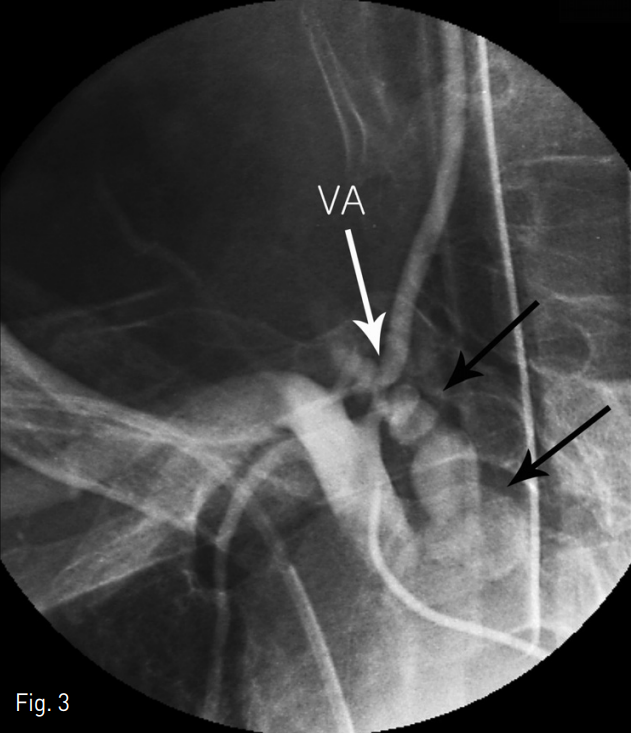
Fig. 3
Selective right subclavian angiography shows the irregular shaped large pseudoaneurysm (black arrows) of the proximal portion of the right vertebral artery (VA)
Fig. 4
Final selective right subclavian angiography revealing no filling of the pseudoaneurysm after coil embolization of proximal ver tebral artery (VA) and stent graft at subclavian artery across the VA origin.
추적관찰
추적검사에서 가성동맥류는 완전히 소실되었으며 환자는 합병증 없이 중환자실에서 잘 치료되었고 퇴원하였다.
고찰
중심정맥 관 삽입술은 응급상황이나 중환자실에서 자주 시행되는 시술이다. 중심정맥관의 종류에 따라서 내경정맥, 쇄골하정맥, 대퇴정맥 등 다양한 정맥들에서 시술될 수 있다. 이중 척추동맥 손상은 드문 합병증이며 보통은 내경정맥 삽입술을 시행하다 발생할 수 있다. 해부학적으로 주사침이 너무 외측이나 깊게 들어갈 경우 척추동맥의 손상을 유발할 수 있다. 보고된 합병증들은 동정맥루, 박리, 혈전증, 가성동맥류 등이 있다. 따라서, 중심정맥관 삽입에 있어 매우 신중을 기하여야 한다. 초음파 유도하 시술이 가능한 추천된다.
참고문헌
1. Momiy J, Vasquez J. Iatrogenic vertebral artery pseudoaneurysm due to central venous catheterization. Proc (Bayl Univ Med Cent) 2011;24(2):96-100.
2. Schummer W, Schummer C, Gaser E, Bartunek R. Loss of the guide wire: mishap or blunder? Br J Anaesth 2002;88(1):144-6.
3. Inamasu J, Guiot BH. Iatrogenic vertebral artery injury. Acta Neurol Scand 2005;112(6):349-57.
4. Ruesch S, Walder B, Tramer MR. Complications of central venous catheters: internal jugular versus subclavian access--a systematic review. Crit Care Med 2002;30(2):454-60.
5. Maruyama K, Nakajima Y, Hayashi Y, Ohnishi Y, Kuro M. A guide to preventing deep insertion of the cannulation needle during catheterization of the internal jugular vein. J Cardiothorac Vasc Anesth 1997;11(2):192-4.
6. Hind D, Calvert N, McWilliams R, Davidson A, Paisley S, Beverley C, et al. Ultrasonic locating devices for central venous cannulation: meta-analysis. BMJ 2003;327(7411):361.
7. Golden LR. Incidence and management of large-bore introducer sheath puncture of the carotid artery. J Cardiothorac Vasc Anesth 1995;9(4):425-8.
Citations
Citations to this article as recorded by