중심단어
Gastrointestinal bleeding, portal vein occlusion, stent placement, varix embolization.
임상소견
5년 전 초기 원위부 담관암으로 유문부 보존 췌십이장 절제 (Pylorus-preserving pancreaticoduo denectomy, PPPD) 받은 환자로 특별한 증상 없이 지내다가 15일 전부터 지속된 하루 한두 차례의 토혈과 혈변을 주소로 내원하였다. 외부병원에서 시행한 내시경에서 출혈 부위를 찾지 못했고 복부 CT에서는 새롭게 발생한 간문맥 혈전과 afferent loop에서 조영제의 유출이 관찰되어 혈관조영술을 시행했으나 출혈 부위는 발견하지 못한 채 Hb 4.8 g/dl인 상태로 전원되었다. 본원에 내원하여 2차례에 혈관조영술을 시행 받았으나 출혈부위는 찾지 못했다.
진단명
Jejunal varix bleeding by cavernous transformation secondary to post-operative portal vein occlusion
영상소견
시술 전 연속적으로 시행한 CT에서 간 문맥 혈전이 점점 증가함에 따라 cavernous transformation이 함께 증가하는 것이 관찰되었으며 전원 직전의 CT에서는 afferent loop에서 조영제의 장내 유출이 관찰되어 active bleeding 상태임을 알 수 있었다. 위, 대장내시 경에서는 경도의 식도 정맥류가 있었고 출혈 부위는 확인하지 못했다. 대퇴부동맥 혈관조영술에서도 출혈부위는 찾을 수 없었다. GI bleeding scan에서는 우상복부에 tracer accumulation 이 지속적으로 관찰되어 afferent loop 출혈에 합당한 소견을 보였다.
Fig. 1. A 78-year-old female who underwent PPPD 5 years ago presented with hematemesis and hematochezia.
A. CT reveals portal vein thrombosis (arrow) and associated cavernous transformation and ascites.
B. Extravasation of contrast media (arrow) in jejunum suggests active bleeding in afferent loop.
시술방법 및 재료
21-gauge needle (Chiba, Cook, IN, USA)로 S6 portal vein을 puncture한 후 4 Fr coaxial dilator로 교체 후 7 Fr long sheath 삽입 후 0.035-inch angled hydro philic stiff guide wire (Radifocus, Terumo, Tokyo, Japan)와 5 Fr catheter (Cobra, Cook, IN, USA)를 이용하여 portal vein의 thrombus를 통과하여 portogram을 시행하였다. SMV와 splenic vein 연결부위에서부터 6 cm에 걸쳐 thrombus에 의한 filling defect가 관찰되었다. 또한
collateral vein에 의한 간문부의 cavernous transformation이 관찰되었다. Thrombus내에 8mm balloon catheter (Synergy, Boston Scientific, MA, USA)을 이용하여 dilatation한 후에도 filling defect가 남아있어 7 Fr McNamara catheter를 이용하여 aspiration thrombectomy를 시행하고 직경 12mm, 길이 8cm의 self-ex panding stent (Zilver, Cook, IN, USA)를 설치하고 portogram을 시행하였다. 그러나 stent가 이전 문맥 문합부에서 angulation을 보이
고 남은 thrombus가 있어 다시 한번 8mm balloon dilatation을 시행 하였다. 정상적인 portal flow가 회복된 후 cavernous transformation의 flow는 감소하
였고 main portal vein에서의 pressure gradient는 24mmHg에 서 13mmHg로 감소하였다. Transhepatic tract을 NBCA로 embolization한 후 검사를 종료하였다. 이후 증상이 호전되어 병상 추적관찰 중 4일 후에 다시 토혈이 시작되어 CT를 촬영하였고 다시 in-stent thrombus가 발견되었으며 공장에서 재출혈이 의심되었다. 다시 S5 portal vein을 puncture 하여 7 Fr sheath insertion후에 5 Fr cobra catheter를 넣고 wire를 portal vein stent내의 thrombus를 통과시킨 후 2.2 Fr microcatheter (Meister, Asahi, Aichi, Japan)를 collateral vein을 따라 jejunum으로 위치하고 시행한 혈관조영에서 jejunum으로 contrast media의 extravasation이 관찰되었다. 그 부분을 microcoil (Nester, Cook, IN, USA) 4개와 gelfoam, NBCA (histoacryl)를 사용하여 embolization을 시행하였고 문맥에는 다시 12mm x 4cm balloon dilatation과 10mm x 4cm의 self-ex panding stent (Epic, Boston scientific, MA, USA) placement하였다. 이후 portogram에서 active bleeding은 차단되었으며 정상적인 portogram이 회복되었다. Transhepatic tract을 NBCA로 embolization하고 검사를 종료하였다.
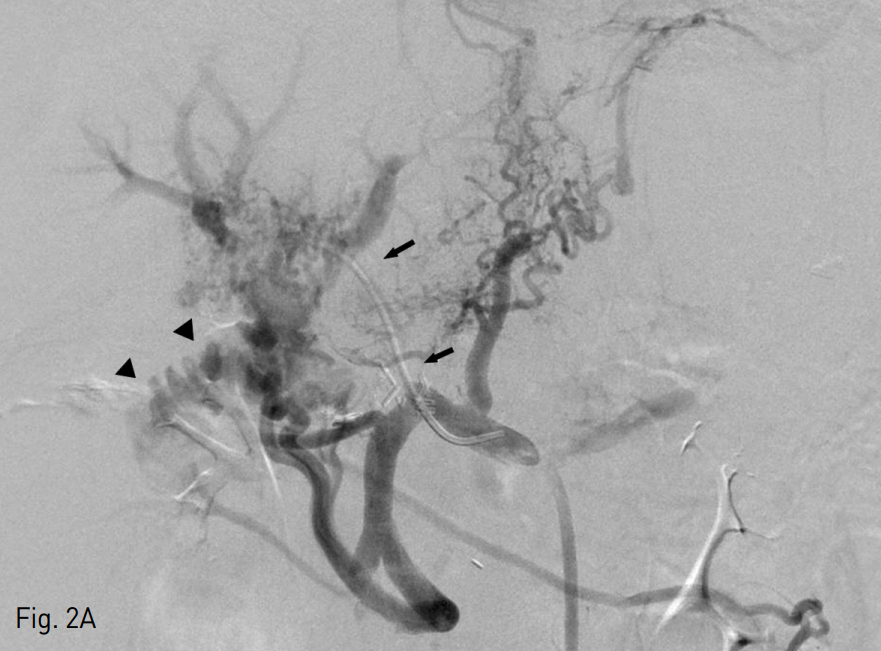
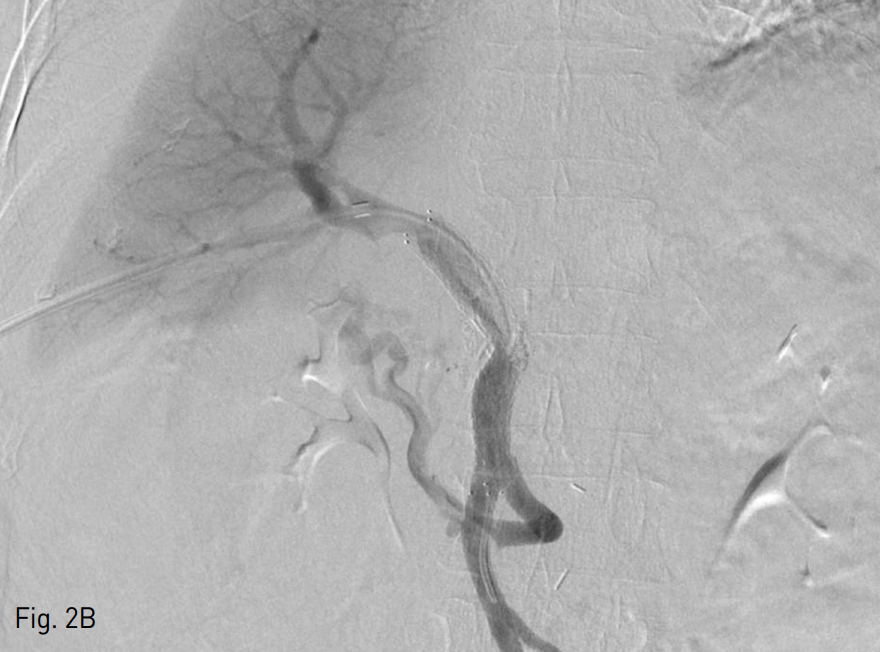
Fig. 2
A. Transhepatic portogram shows filling defect in portal vein (arrows), suggestive of thrombus and extravasation of contrast media (arrowheads) to jejunum.
B. Balloon dilatation, thrombectomy, and stent placement restored portal vein flow and decreased collateral flows.
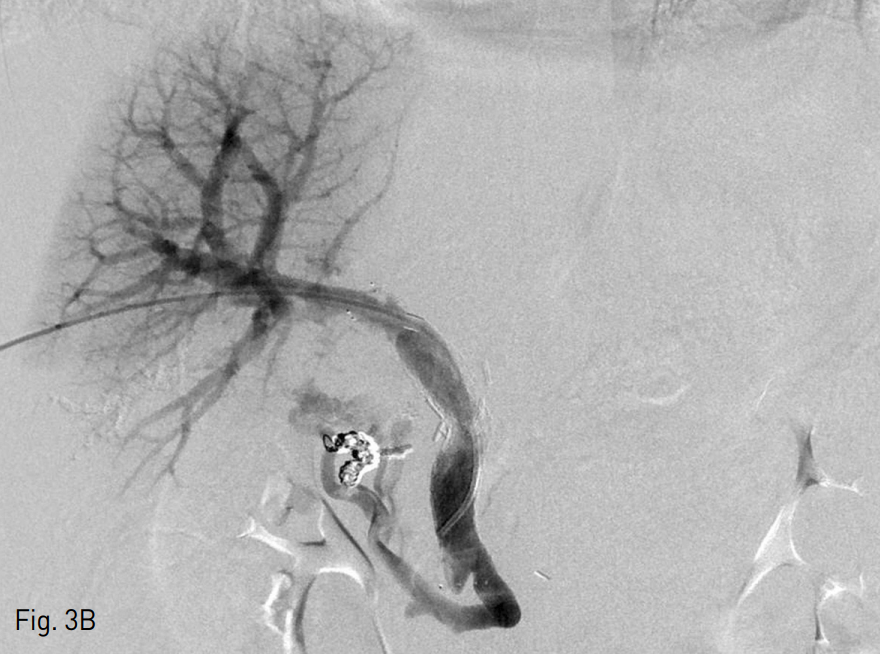
Fig. 3
A. Second transhepatic portogram with microcatheter shows active contrast media leakage to jejunum (arrows)
B. Seletive embolization with microcoils and recanalization with balloon dilation and stent placement were performed and portogram shows some residual cavernous transformation and patent portal vein flow.
추적관찰
이후 시행한 CT에서 cavernous transformation은 감소하였고 portal vein의 partial thrombus가 있으나 portal hypertension관련된 bowel edema, ascites, effusion 등은 모두 호전되었다. 환자는 임상증상이 호전되어 퇴원하였다. (검사소견 Hb 10.2g/dl, AST 30IU/L, ALT 23 IU/L, Total bilir ubin 0.3mg/dL)
고찰
췌십이지장 절제술후 간문맥 폐쇄에 의한 공장 출혈은 드문 증례이다. 만성 간경화에 의한 간문맥 고혈압의 경우 식도 또는 위 정맥류 출혈로 발현하는 경우가 많으나 문맥혈전에 의한 경우 전형적으로 gastrohepatic ligament의 paracholedocal and epicholedochal vein의 dilatation인 cavernous transformation이 발생한다. PPPD 수술의 경우 문맥 절제 및 문합 부위에 방사선치료 또는 악성종양의 재발로 문맥혈전이 흔히 발생할 수 있으며 공장을 거쳐 cavernous transformation과 연결되는 측부순환에서 공장정맥류 출혈로 드물게 나타날 수 있다 (1-4). 본 증례의 경우 공장으로 afferent loop를 길게 만들어 내시경으로 출혈 부위를 확인 할 수 없었으며 CT에서 출혈부위가 확인되었으나 문맥계 출혈로 동맥 조영에서도 출혈을 확인할 수 없었다. 이러한 경우 정확한 진단이 어려우나 췌십이장 절제술 후 출혈부위를 찾을 수 없는 환자에서 문맥계 출혈을 의심할 수 있으며 그런 경우 반복적인 내시경과 혈관조영술을 피할 수 있을 것으로 생각한다.
처음 시행한 경간 간문맥 혈관조영술에서 간문맥 재개통 만으로 충분할 것으로 생각했으나 4일 만에 문맥혈전이 재발하여 다시 같은 양상의 출혈이 발생하였다. 이전 연구에서 간문맥 재개통만으로 측부순환이 충분히 감소하는 경우 대부분 출혈이 멈추고 재발하는 경우가 드물었다. 그러나 문맥이 혈류가 완전히 회복되지 않은 상태에서 풍부하게 형성된 측부 순환이 있는 경우 문맥혈류가 다시 감소하여 혈전발생과 공장출혈이 재발된 것으로 생각된다. 이 때 출혈부위 측부순환을 일부 차단하는 것이 도움이 되었으며 측부 순환을 완전히 차단하는 것 보다는 선택적으로 출혈 혈관 색전하는 것이 간기능 유지에도 도움이 될 것으로 생각한다. 이 환자에서 간수치는 시술 전후에서 안정적으로 유지되었다.
PPPD 이후 공장 출혈환자에서 간문맥혈류 재개통만으로도 출혈을 충분히 조절할 수 있을 것으로 보이나 severe fibrosis 혹은 재발로 인해 문맥 재개통을 충분하지 못한 경우 일부 측부순환 색전을 함께 고려해야 할 것으로 생각된다.
참고문헌
1. 현동호, 신성욱, 조성기, 등. PPPD 후 간문맥폐쇄에 의해 발생한 공장 정맥류의 성공적 치료. 대한인터벤션영상의학회지 2014;21:159-16 2.
2. Hwang S, Sung KB, Park YH, Jung DH, Lee SG. Portal vein stenting for portal hypertension caused by local recurrence after pancreatoduodenectomy for periampullary cancer. J Gastrointest Surg 2007;11:333-337.
3. Kim KR, Ko GY, Sung KB, et al. Percutaneous transhepatic stent placement in the management of portal venous stenosis after curative surgery for pancreatic and biliary neoplasms AJR 2011;196:w446-w450.
4. Shimizu Y, Yasui K, Fuwa N, Arai Y, Yamao K. Late complication in patients undergoing pancreatic resection with intraoperative radiation therapy: gastrointestinal bleeding with occlusion of the portal system. J Gastroenterol 2005;20:1235-1240
Citations
Citations to this article as recorded by