중심단어
Arterioureteral fistula, pseudoaneurysm, arteriography, retrograde ureterography, embolization
임상소견
A 64-year-old woman, who previously had multiple lumbar disc operations up till 6 years ago, presented to our institution with history of gross hematuria. The patient had multiple metal
plates for posterolumbar fixation and there was anterior protrusion of the artificial disc placed at the level of L4/5.The CT scan showed a left ureteral stricture with hydronephrosis, and the patient underwent left radical nephroureterectomy. Nine months later, the patient presented again with gross hematuria. The cystoscopy showed left lateralizing hematuria, but the CT urography showed no evidence of postoperative complication at the left nephrectomy site.
진단명
Arterioureteral fistula
영상소견
An angiography was attempted in order to localize a bleeding focus. It showed an occlusion of left common iliac artery (CIA) with a bulging contour at the occlusion site suggesting the presence of a pseudoaneurysm abutting the fixation metal of the lumbar vertebra (Fig. 1). The angiography was attempted via lumbar, right internal iliac and inferior mesenteric artery, and did not show a bleeding focus. The left renal artery stump at the left nephrectomy site was intact. A venogram via right femoral vein did not demonstrate abnormal communications. Hence, the angiography failed to identify a definite bleeding focus to account for gross hematuria.
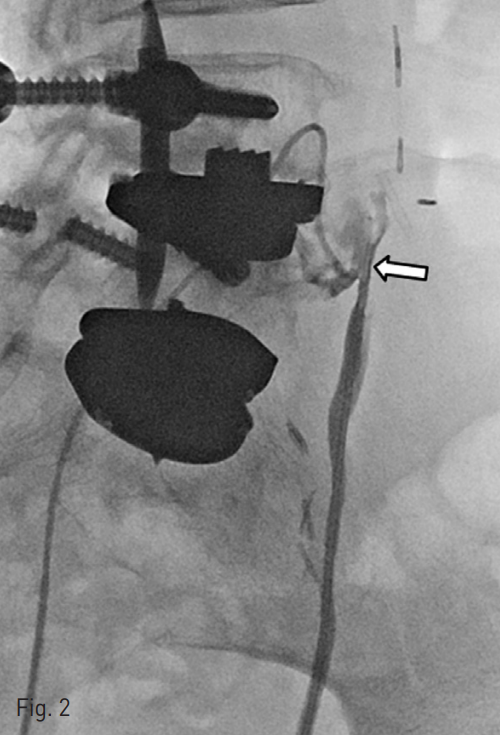
Subsequently, retrograde ureterography was performed and revealed a potential communication between the ureteral stump and left CIA occlusion site pseudoaneurysm. A repeat angiography was performed and microcatheter was inserted via left CIA. The contrast medium was injected via the remnant left ureter, and the fistulous tract was successfully identified and negotiated with the microcatheter into the remnant left ureter (Fig.2).
Fig. 1
The angiography shows an occluded left CIA and a bulging vascular structure (arrows) behind the metal plate that is most likely to represent a pseudoaneurysm at the occlusion site
Fig. 2
The retrograde ureterography reveals a potential communication (arrow) between the ureteric stump and left CIA occlusion site pseudoaneurysm.
시술방법 및 재료
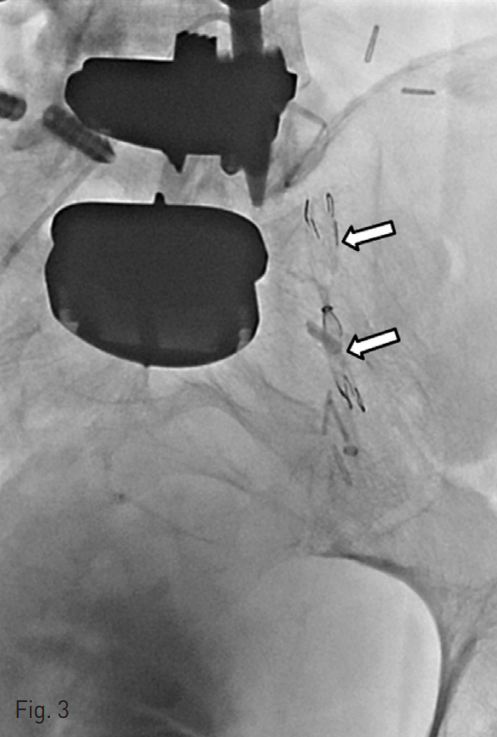
Prior to embolization of the fistulous tract, we decided to place a ureteral occlusion stent in the remnant left ureter in order to prevent the spillage of embolic material into the bladder (Fig. 3). The ureteral occlusion stent (S&G Biotech; Seongnam, Gyunggi-do, Korea) was internally coated with a thin silicone membrane with the central portion completely obstructed in a candy-wrapper configuration.
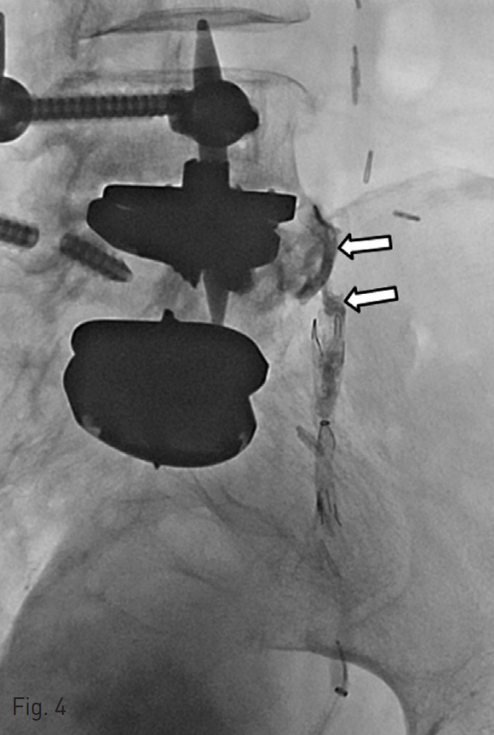
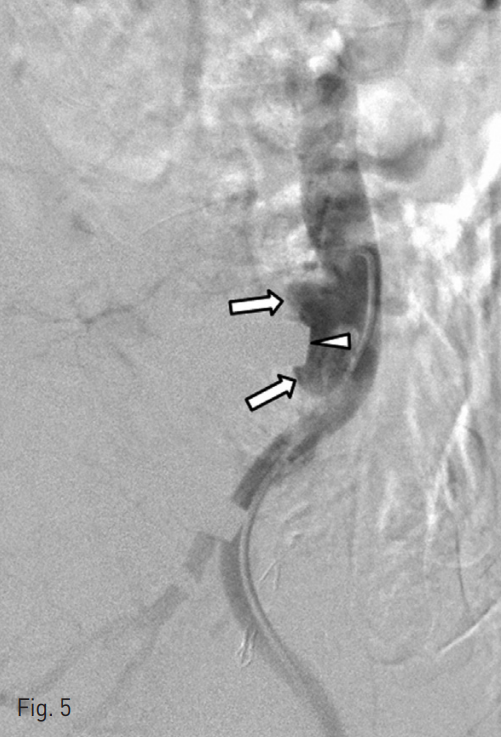
Then, we used N-butyl cyanoacrylate glue (n-BCA, 1 : 3, total 3cc) material to embolize the fistulous tract via microcatheter in left CIA occlusion site pseudoaneurysm (Fig. 4). The postembolization angiogram confirmed the obliteration of the fistulous tract (Fig. 5).
Fig. 3
The ureteral occlusion stent (arrows) was deployed in the left remnant ureter in order to prevent the spillage of embolic material into the bladder prior to embolization.
Fig. 4
The fistulous tract between the left CIA occlusion site pseudoaneurysm and ureteric stump was embolized using N-BCA (arrows).
Fig. 5
The lateral aortography after embolization shows pseudoaneurysm-like bulging (arrows) of the distal aorta and the obliteration of the fistulous tract. Note the indentation (arrowhead) of the bulging against the metallic plate
추적관찰
At three months follow up, the patient reported occasional mild hematuria, although gross hematuria resolved.
고찰
Arterioureteral fistula is an uncommon but potentially life-threatening cause of hemorrhage. Approximately 85% of arterioureteral fistulas are secondary and occur following pelvic surgeries. The presence of a ureteral stump after nephrectomy is recognized as a predisposing condition to the development of arterioureteral fistulas (1). The occlusion of CIA and presence of pseudoaneurysm at the occlusion site are also likely to have contributed to formation of arterioureteral fistula in our case. Although the pathophysiology leading to the development of arterioureteral fistula is not well established, ischemic or inflammatory injuries to the ureters or iliac vessels are thought to have played a major role, particularly following repeated intra-abdominal and pelvic operations as in our patient.
The diagnosis of arterioureteral fistula may be challenging due to the difficulty in confirming the fistulous communications using radiology. In our patient, iliac arteriography was performed first in an attempt to identify the bleeding focus. The angiography revealed an occlusion of left CIA likely secondary to the multiple previous lumbar disc operations. At the time, it was not readily appreciated the presence of pseudoaneurysm at the occlusion site but the ocdusion site appeared bulging rather than tapering as one would expect for a stenosis. A bleeding focus or fistulous tract was not identified with arteriography. As an alternative approach, retrograde ureterography was attempted and enabled the identification of the potential fistulous tract and the tract was selected via microcatheter inserted to the left CIA.
Selective iliac arteriography is considered the most sensitive technique in diagnosing arterioureteral fistula, but its sensitivity rate is less than 50% (2). It may be due to the fistula being occluded by a thrombus during quiescent times. Provocation maneuvers such as high-pressure balloon occlusion pyeloureterography may be used to actively dislodge the thrombus. Also, obtaining multiple oblique projections may help identifying small pseudoaneurysms that may otherwise be overlooked. In our patient, the metal plates from previous lumbar disc operations made it difficult to appreciate the presence of pseudoaneurysm at the occlusion site and obtaining oblique projections could have assisted in readily detecting the pseudoaneurysm.
Ureteral occlusion stent has been described for use inpostoperative ureteral leak (3). The nitinol stent frame internally coated with silicone membrane was constructed in a candy-wrapper configuration with its central portion completely obstructed. This enabled the stent to be completely watertight and served to prevent the spillage of embolic material into the bladder. The expansile nature of the nitinol stent frame allowed stable anchoring within the ureter with its bare metallic portions at both ends for peripheral attachment by tissue ingrowth.
N-BCA has been previously utilized as an embolic material for visceral artery pseudoaneury sm (4). N-BCA has a liquid property and low viscosity, which enables embolization of complex shaped and tortuous vessels with abundant collateral vessel formation. It has also been reported as an agent for ureteric embolization (5). N-BCA solidifies rapidly but may soften, migrate, fragment or recanalize with time, and appropriate follow up may be necessary.
In this report, we present an unusual case of arterioureteral fistula between ureteral stump following nephroureterectomy and arterial pseudoaneurysm at its occlusion site. The identification of the fistulous tract was achieved via retrograde ureterography rather than angiography. The ureteral occlusion stent was used to prevent the spillage of embolic material, and the fistulous tract was embolized using N-BCA.
참고문헌
1. Bergqvist D, Parsson H, Sherif A. Arterio-ureteral fistula--a systematic review. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2001;22(3):191-6.
2. Vandersteen DR, Saxon RR, Fuchs E, Keller FS, Taylor Jr LM, Barry JM. Diagnosis and Management of Ureteroiliac Artery Fistula: Value of Provocative Arteriography Followed by Common Iliac Artery Embolization and Extraanatomic Arterial Bypass Grafting. The Journal of Urology. 1997;158(3):754-8.
3. Park HJ, Shin JH, Kim JW, Hong BS. Postoperative Ureteral Leak Treated Using a Silicone-Covered Nitinol Stent. International Neurourology Journal. 2015;19(1):47-50.
4. Won Y, Lee SL, Kim Y, Ku YM. Clinical efficacy of transcatheter embolization of visceral artery pseudoaneurysms using N-butyl cyanoacrylate (NBCA). Diagnostic and interventional imaging. 2015.
5. Saad WE, Kalagher S, Turba UC, Sabri SS, Park AW, Stone J, et al. Ureteric embolization for lower urinary tract fistulae: use of two amplatzer vascular plugs and N-butyl cyanoacrylate employing the "sandwich" technique. Cardiovascular and interventional radiology. 2013;36(4):1068-72.
Citations
Citations to this article as recorded by