중심단어
Systemic artery to pulmonary artery shunt, embolization, percutaneous, transarterial
임상소견
64세 남자 환자가 입인두암 수술, 동시 항암화학방사선 요법 후 경과 확인을 위한 흉부 CT에서 발견된 이상소견으로 내원했다. 흉부 CT에서 좌상엽 첨후분절에 폐동맥과 체동맥(왼쪽 쇄골하동맥의 분지 및 늑간동맥) 사이의 교통으로 인해 늘어난 혈관 구조물이 발견되었다. 환자는 평소 호흡기적 증상이나 흉부 불편감은 었다. 기저질환으로는 고혈압, 당뇨가 있었고. 그외 다른 특이질환은 없었다.
영상소견
흉부 CT 검사상 좌상엽 첨후분절에 체동맥(왼쪽 쇄골하동맥의 분지와 늑간동맥)과 폐동맥 사이의 교통으로 인해 늘어난 혈관 구조물이 관찰되었다(Fig. 1A). 흉부 CT 영상의 3차원 재구성 기법(maximum intensity projection and volume rendering technique)을 이용한 영상에서 왼쪽 쇄골하동맥과 폐 동맥 분지 사이의 교통을 더 명확하게 볼 수 있었다 (Fig. 1B-C). 이 병변으로 인한 특별한 호흡기 증상은 보이지 않았으나 파열에 의한 출혈의 위험성이 있는 것으로 생각하고 색전술을 하기로 결정하였다.
Fig. 1
A. Contrast enhanced chest CT shows tortuous dilated intrapulmonary vascular structure in left upper lobe apicoposterior segment (arrow).
B, C. Maximum intensity projection image of the chest CT shows tortuous dilated intrapulmonary vascular structure in left upper lobe apicoposterior segment (arrow) and tortuously dilated systemic vessels in the chest wall (arrow heads).
D. Volume rendering image of chest CT shows left 3rd intercostal artery (arrow) to pulmonary artery (curved arrow) fistula. The intercostal artery shows hypertrophy, and tortuosity.
시술방법 및 재료
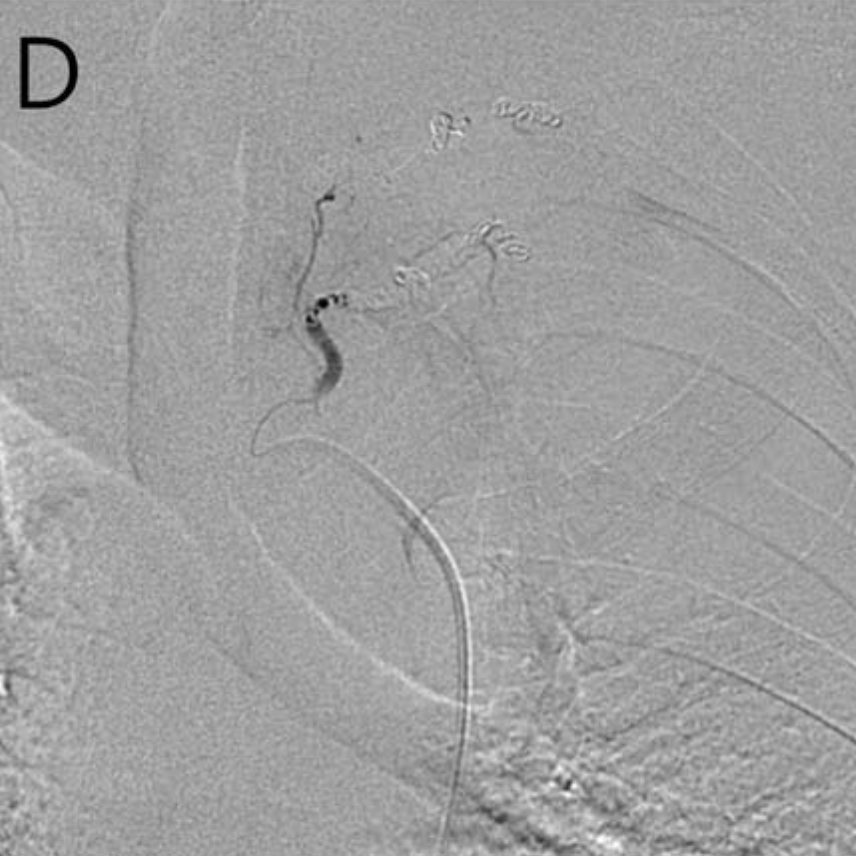
초음파 유도 하에 우측 대퇴동맥을 천자하여 5-Fr vascular sheath를 삽입하고 sheath를 통해 5-Fr Headhunter catheter를 왼쪽 쇄골하동맥 기시부에 거치시켰다. 왼쪽 쇄골하동맥 조영술을 시행하여 폐 좌상엽 첨후분절에 갑상목동맥에서 분지하는 체동맥-폐동맥단락과 이로 인해 확장된 혈관 구조물을 확인할 수 있었다. 미세카테터를 이용하여 초선택 (superselection)하여 혈관조영술을 시행하였을 때 혈관확장, 꼬부라짐(tortuosity), 미세 기형혈관(fine malformed vessels), 동정맥 단락(arteriovenous shunt) 소견이 보였다(Fig. 2A). 갑상목동맥의 몇 개의 분지가 이러한 소견을 보였고 이 분지들은 좌상엽 첨후분절의 폐동맥과 연결을 보였다. 각각의 분지를 미세카테터를 이용하여 초선택 하였고 여러 개의 미세코일 (Tornado Embolizalion Coil, Cook medical, USA)을 이용하여 색전술을 시행하였다(Fig. 2B). 다음으로 5-Fr Headhunter catheter를 이용하여 왼쪽 3번째 늑간동맥을 선택하여 동맥 조영술을 시행했다. 역시 혈관확장, 꼬부라짐(tortuosity), 미세 기형혈관(fine malformed vessels), 동정맥 단락(arteriovenous shunt) 소견이 보였고 좌상엽 첨후분절의 폐동맥과 연결되어 있었다. 늑간 동맥은 좌상엽 첨후분절의 폐동맥과 연결을 보였다(Fig. 2C). 미세카테터를 이용하여 초선택 하였고 여러 개의 미세코일(Tornado Embolization Coil, Cook medical, USA)을 이용하여 색전술을 시행하였다(Fig. 2D). 시술 후 시행한 동맥 조영술에서 좌상엽 첨후분절의 체동맥-폐동맥루 는 보이지 않는 것을 확인했다.
Fig. 2
A. Conventional angiography of the feeding branch of the thyrocervical trunk via microcatheter shows systemic to pulmonary shunt. The feeding systemic artery (arrow) shows slight hypertrophy and tortuosity, and drains into the pulmonary artery (curved arrow) via multiple file malformed vessels (arrow heads) in the left upper lobe.
B. Angiography of the thyrocervical trunk after embolization shows no residual systemic to pulmonary artery shunt.
C. Angiography of left 3rd intercostal artery (arrow) shows tortuosity, slight hyper trophy and multiple fine malformed vessels (arrow heads) draining into the pulmonary artery (curved arrow) in the left upper lobe.
D. Angiography of the intercostal artery after embolization shows no residual systemic to pulmonary artery shunt.
고찰
체동맥- 폐동맥부는 비정상적 혹은 비대한 체동맥과 폐동맥 간의 교통을 말한다. 이러한 동맥 기형은 보통 늑간동맥, 내유동맥(internal manmary artery), 기관지동맥, 아래가로막동맥 등과 폐동맥 사이에서 일 어나는데 선천적, 후천적 발생이 모두 가능하다고 알려져 있다. 후천적 체동맥-폐동맥루의 발생요인으로는 미숙아 출생, 선천적 심장 질환, 만성 폐 감염, 악성 신생물, 외상 등이 있을 수 있다. 선천적 체동맥-폐동맥루는 건강한 1개월 유아를 대상으로 조사했을 때 1.57%의 유병률을 보였다. 이러한 체동맥-폐동맥루는 두 가지 그룹으로 나뉠 수 있다. 첫째는 선천성 청색증형 심장질환으로 인해 동맥이 작은 경우 폐문주변과 폐 내부의 체동맥과 폐동맥이 연결되어 커다란 단락을 이루는 것이다. 둘째는 대동맥과 그 분지들 여러 곳 에서 폐동맥과 일부 연결되어 작고 구불구불한 형태로 보이는 혈관 병변이다.
체동맥- 폐동맥루는 대체로 무증상이나 누공을 통한 감염의 급속한 전파, 출혈로 인한 객혈, 폐동맥 고혈 압을 유발할 경우 심장과 관련된 합병증 등을 일으킬 수 있다. 체동맥-폐동맥루의 자연경과는 잘 알려져 있지 않으며 치료를 위한 정확한 적응증도 마련되어 있지 않다. 하지만 현재 무증상 환자더라도 나중에 일어 날 수 있는 위와 같은 합병증을 대비해 치료가 필요하다는 주장이 있다. 효과적이고 올바른 치료 방법이 무 엇인가에 관해서도 여전히 논란이 있다. 누공과 함께 동맥루로 인한 혈관 병변이 포함된 폐실질을 엽절제와 같은 수술로 제거하고 혈관의 입구를 막는 것이 현재 가장 확실한 치료로 생각되고 있다. 그러나 최근 색전 술이 수술과 전신마취의 위험성을 줄이는 좋은 치료라는 주장이 있다. 특히 출혈로 인한 객혈증상이 나타날 경우 색전술이 가장 먼저 시도될 수 있는 비교적 안전하고 검증된 치료라는 점, 여러 분지의 체동맥에서 혈 액을 공급받는 병변의 경우 동맥조영술로 구조를 정확하게 파악하고 모두 시술 가능하다는 점을 주목해야 할 것이다. 여러 개의 체동맥으로부터 혈액공급을 받는 체동맥-폐동맥루를 가진 환자에서 본 증례처럼 여러 차 례의 미세코일 색전을 이용해 성공적으로 치료한 증례가 보고되어 있으나 매우 드물다. 이전 증례 보고에서 색전 시술 도중 급성 소뇌 경색이 나타났던 증례가 있다. 신경학적 지연성 후유증을 남기지는 않았으나 폐동 정맥루의 색전 시술에서처럼 색전 시술 후 신경학적 증상에 관해 주의를 기울일 필요가 있을 것으로 생각된다. [1-7]
참고문헌
1. Yu CH, Chen MR. Clinical investigation of systemic- pulmonary collateral arteries. Pediatr Cardiol. 2008; 29(2):334-8
2. Lee JK, Park JH, Kim J, Kim SJ, Lee AR, Lee CH, et al. Embolization of multiple systemic artery to pulmonary artery fistula with recurrent hemoptysis. Tuberc Respir Dis (Seoul). 2013; 75(3):120-4
3. Morais F, Almeida T, Campos P. Arterio-arterial fistula between pulmonary and intercostal arteries-case report of “unilateral rib notching”. Rev Port Pneumol (English Edition). 2014;20(3):167-71.
4. Cantasdemir M, Kantarci F, Islak C, Kocer N, Saltuk L, Numan F. Transcatheter coil embolization of an intercostal artery to pulmonary artery fistula. Eur Radiol 2002;12(2):454-7.
5. Jefferson K, Rees S, Somerville J. Systemic arterial supply to the lungs in pulmonary atresia and its relation to pulmonary artery development. Br Heart J. 1972;34(4):418.
6. Itano H, Lee S, Kulick DM, Iannettoni MD, Williams DM, Orringer MB. Nontraumatic chest wall systemic-to- pulmonary artery fistula. The Annals of thoracic surgery. 2005;79(5):e29-e31.
7. Yon JR, Ravenel JG. Congenital bronchial artery- pulmonary artery fistula in an adult. J Comput Assist Tomogr 2010;34(3):418-20.
Citations
Citations to this article as recorded by