중심단어
Transjugular intrahepatic portosystemic shunt, recananlized paraumbilical vein, liver cirrhosis, portal hypertension
임상소견
알코올성 간경변 환자가 내원 전일 발생한 hematemesis를 주소로 내원하였다. Levin tube irrigation에서 fresh active bleeding이 확인되었고, 환자는 gastric varix로 sclerotherapy를 2회 시행받은 병력이 있었다. 환자는 응급 내시경을 시행하여 tortuous dilatated esophageal varix를 확인하였고 혈관 결찰술을 시행하였다. 그러나 이후에도 melena, 혈색소의 감소, 혈압저하 등의 출혈소견이 계속 보여서 gastric, esophageal varix의 치료 목적으로 transjugular intrahepatic portosystemic shunt (TIPS)를 고려하였다. 시술 전 평가를 위해 시행한 Liver CT에서 상복부의 복벽에서 간좌엽 문맥으로 연결되는 recanalized paraumbilical vein을 확인하였다.
진단명
Esophageal variceal bleeding in alcoholic liver cirrhosis
영상소견
상부위장관 내시경에서 esophageal varix의 출혈소견이 확인되었고 내시경적 결찰술을 시행하였다(Fig. 1). TIPS 시술 전 평가를 위해 시행한 Liver CT에서 recanalized paraumbilical vein이 확인되었다(Fig. 2A, B).
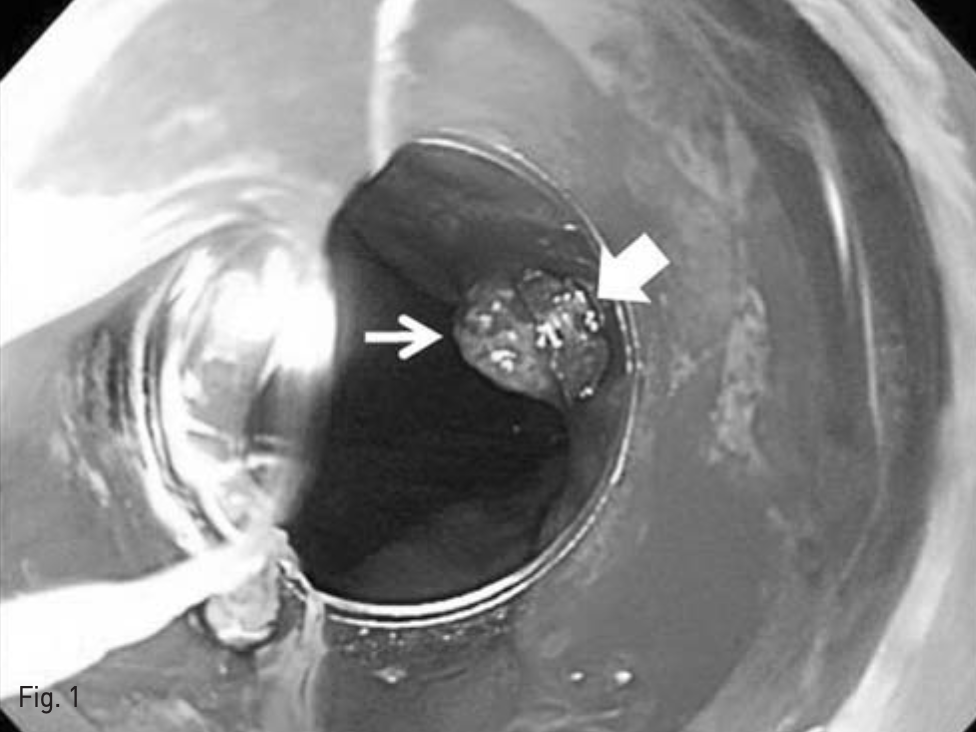
Fig. 1
Esophagogastroduodenoscopy and vascular ligation. Active esophageal variceal bleeding was noted (thin arrow).
Endoscopic vascular ligation was done for esophageal variceal bleeding (thick arrow).
Fig. 2
Liver dynamic CT for preprocedural evaluation
A. Venous phase CT image revealed dilated recan alized paraumbilical vein in abdominal wall (arrow)
B. This recan alized paraumbilical vein drains left portal vein (arrow).
시술방법 및 재료
복벽에 확장되어 있는 recanalized paraumbilical vein을 초음파 유도하에 천자하여(Fig. 3), 왼쪽 문맥 으로 5-Fr 카테터를 삽입하였다. 문맥조영술을 시행하여 간내문맥을 확인하였다. Right intrnal jugular vein을 천자하여 5-Fr 카테터를 삽입하여 오른쪽 간정맥 조영술을 시행하고 오른쪽 간정맥을 신택한다. 이후 recanalized paraumbilical vein을 통한 문맥조영술 을 roadmap으로 이용하여 16G Colapinto needle (Cook Inc, Bloominglon, IN, USA) 오른쪽 간문맥을 천자하였다(Fig. 4). 천자된 경로를 6mm x 4cm balloon (Mustang, Boston Scientific, Massachusetts, USA)을 이용하여 확장하고, 10mm x 5cm partially covered stent (Niti-s TIPS Stent, Tae Woong medical, Gyeonggi-do, Korea)를 간문맥과 중간간정맥 샛길에 삽입하였다. 이후 스테트가 펴지지 않은 부분을 펴기위해 10mm x 4cm balloon (Mustang, Boston Scientific, Massachusetts, USA)을 이용해 확장하였다. TIPS stent를 설치한 후 시행한 문맥조영술에서 식도정맥류를 보이지 않았고 stent를 통한 원활한 혈류를 확인 할 수 있었다(Fig. 5). 문맥의 평균압력이 시술 전 22mmHg에서 시술 후 14mmHg로 감소하였고, 최대 정맥문맥 압력차이가 16mmHg에서 1mmHg로 감소하였다.
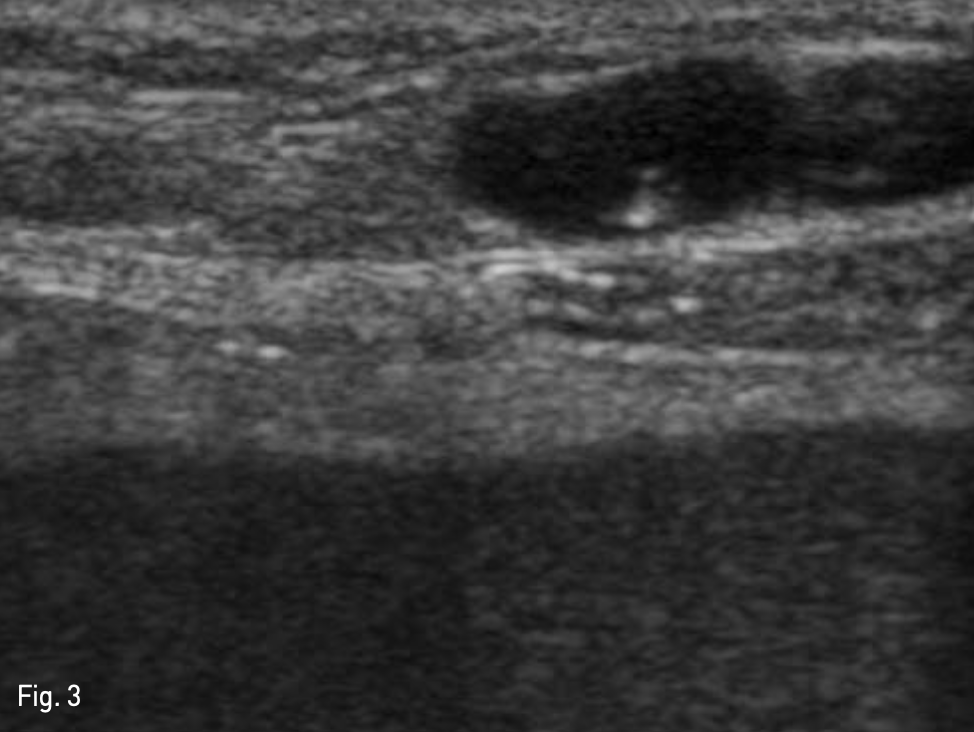
Fig. 3
Puncture of recanalized paraumbilical vein. US guided recanalized paraumbilical vein puncture was done for catheter insertion for portography which is assisted TIPS by visualization of anatomy of portal vein.
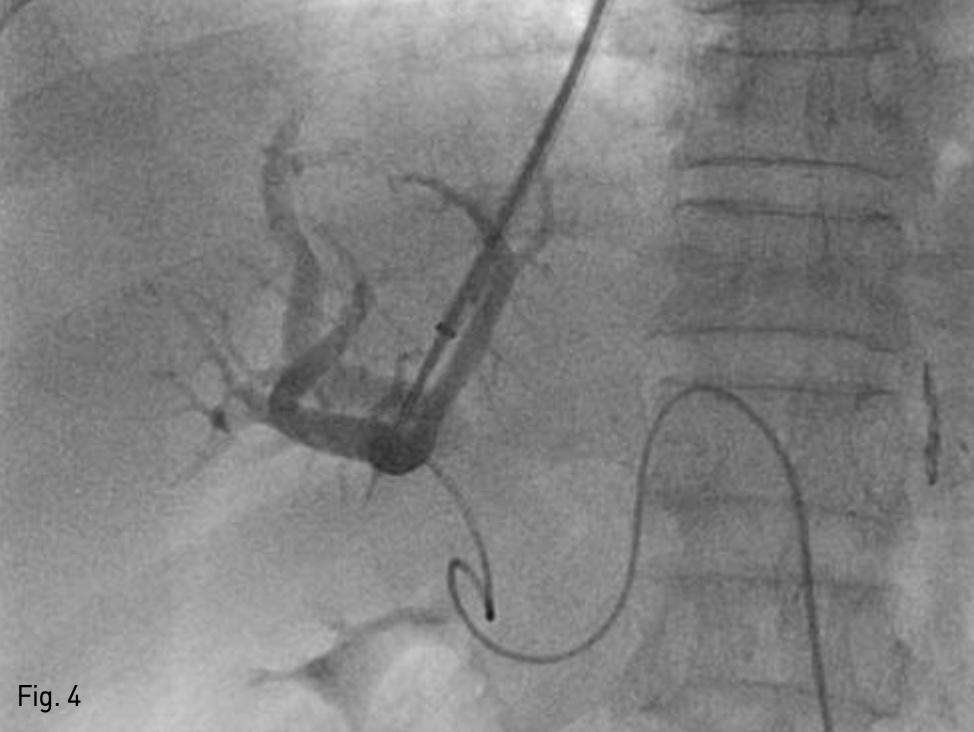
Fig. 4
Right portal vein puncture assisted by paraumbilical vein. Successful puncture of portal vein was done with portogram assisted by recanalized paraumbilical vein.
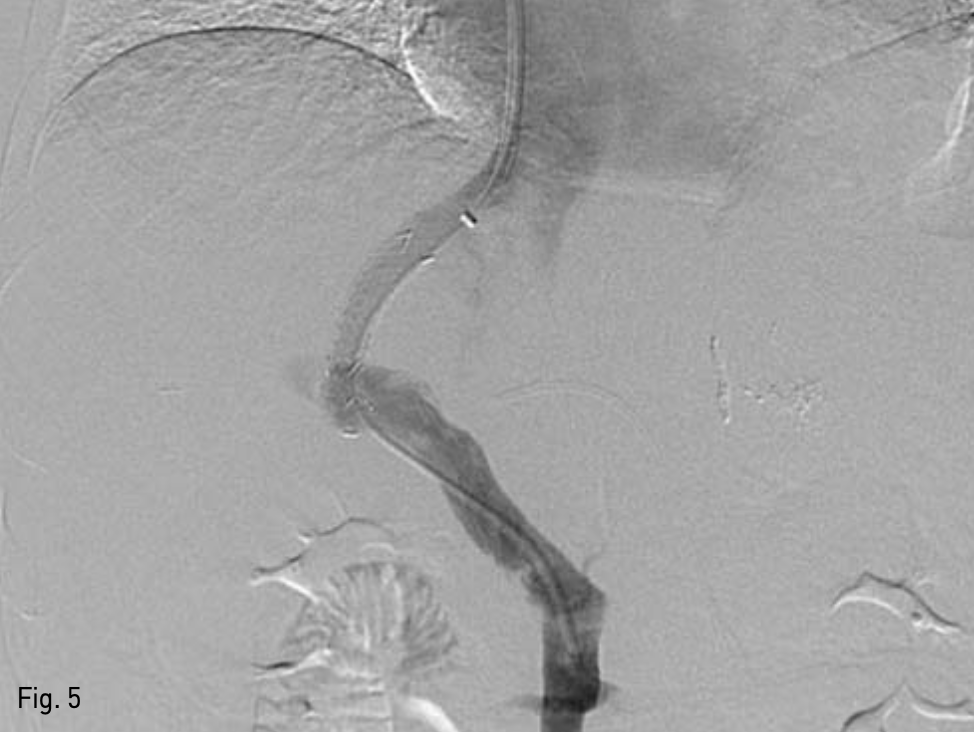
Fig. 5
Stent placement. 10mm x 3.5cm covered x 0.5 and 1.0cm bare metal stent; Niti-S TIPS Stent insertion was done.
추적관찰
시술 후 hematemesis, melena는 확인되지 않았고 Hb은 9.2에서 11.5로 상승하였다. 그리고 생체징후가 안정화되었다.
고찰
TIPS는 간을 경유하여 문맥의 천자를 시도하는 시술로서, 문맥천자 자체에 의한 morbidity, mortality가 있다. 문맥의 위치에 대한 정보는 간 경유 천자횟수를 감소시켜 morbidity, mortality를 감소시킬 수 있는 데, 문맥을 확인하기 위한 다양한 기술적인 방법들이 시도되어 왔다. 문맥을 확인 하기 위한 방법으로는 pre-TIPS 영상(CT, MRI, MR angiography), bony
landmark를 이용하는 방법이 있으며 그 외에도 비침습적인 방법으로는, wedge hepatic venography, intra-parenchymal injection of CO2, wire via inilial transjugular punclure tract as a punclure target, existing stent from old TTPS 방법들도 있다. Wedge venography는 최소한의 기구를 이용하여 다른 술기 없이 쉽고 빠르게 이용할 수 있는 방법으로 가장 흔하게 이용된다. CO2와 Balloon occlusion 카테터를 이용하면 보더 더 문맥을 잘 확인할 수 있지만 카테터에 의한 간피막의 파열이 발생한 증례들이 보고되어 있다.
Recanalized paraumbilical vein catheterization, percutaneous portal catheters, arterial guidance 와 같은 침습적인 방법을 이용하여 intraprocedural portography를 시행 할 수 있다. Percutaneous portal 카테터는 가장 침습식인 방법으로 시술시간이 길고 TIPS를 시행하는 대부분의 환자들은 liver cirrhosis, ascites, coagulapathy가 있고, 기술적인 이려움과 출혈과 같은 합병증을 야기시킬 위험이 있다.
Direct recanalized paraumbilical vein천자를 이 용한 TIPS는 1992년 Wenz F에 의해 처음 보고되었 다. CT나 MRI 등의 시술 전 영상기술이 향상되면서 liver cirrhosis환자에서 recanalized paraumbilical vein이 흔하게 보고되고 있고, 초음파 유도하에 abdominal wall의 recanalized paraumbilical vein을 천자하여 주간문맥에 카테터를 삽입하여 간정맥을 동한 문맥천자를 유도한다. Recanalized paraumbilical vein은 복강내가 아닌 복벽의 정맥으로 복강 내 출혈의 위험도가 낮고 출혈 발생시 쉽게 압박 할 수 있다.
2010년 Matter 등은 114명의 TIPS 시행예정 환자 중 22명의 recanalized paraumbilical vein을 확인하였고 14증례에서 recanalized paraumbilical vein을 이용하여 TIPS에 성공하였다. Recanalizcd paraumbilical vein을 이용한 성공적인 문맥조영술을 위해서는 직절히 굵은 혈관 직경이 요구되고 중등도 이 상의 vascular tortuosity가 없어야 한다.
본 증례는 적절하게 확장된 recanalized paraumbilical vein을 동한 문맥조영술을 이용하여 간경유 문맥 천자 횟수를 최소화 하여 쉽게 portosystemic shunt를 성공적으로 마친 증례로서 의의가 있다.
참고문헌
1. Matthew S. Chin, Joseph M. Stavas, Charles T. Burke, Robert G. Dixon, Matthew A. Mauro. Direct puncture of the recanalized paraumbilical vein for portal vein targeting during transjugular intrahepatic portosystemic shunt procedures: assessment of technical success and safety. J Vas Interv Radiol 2010;21:671-676.
2. Rees CHR, Niblett RL, Lee SP, Diamond NG, Crippin JS. Use of carbondioxide as a contrast medium for transjugular intrahepatic portosystemic shunt procedures. J Vasc Interv Radiol 1994;5:383?386.
3. Martínez-Cuesta A, Elduayen B, VivasI, Delgado C, González-Crespo I, BilbaoJI.CO(2) wedged hepatic venography:technical considerations andcomparison with direct and indirect
4. Morin C, Lafortune M, Pomier G,Robin M, Breton G. Patent paraumbilical vein: anatomic and hemodynamic variants and their clinical importance.Radiology 1992; 185:253-256.
5. Davis AG,Haskal ZJ. Extrahepatic portal vein puncture and intra-abdominal hemorrhage during transjugular intrahepatic portosystemic shunt creation. J Vasc Interv Radiol 1996; 7:863-866.
Deso S, Ludwig B, Kabutey NK, Kim D, Guermazi A. Lymphangiography in the diagnosis and localization of various chyle leaks. Cardiovasc Intervent Radiol 2012;35:117-126.
6. SembaCP, Saperstein L, Nyman U, Dake MD. Hepatic laceration from wedged venography performed before transjugular intrahepatic portosystemic shunt placement. J Vasc Interv Radiol 1996;7:143-146.
7. Theuerkauf I, Strunk H, Brensing KA, Schild HH, Pfeifer U. Infarction andlaceration of liver parenchyma causedby wedged CO(2) venography beforetips insertion. CardiovascInterventRadiol2001; 24:64-67.
8. Brountzos EN, Alexopoulou E, KoskinasI, Thanos L, Papathanasiou MA, Kelekis DA. Intraperitoneal portal vein bleeding during transjugular intrahepatic portosystemic shunt: treatment with stent-graft placement. AJR Am J Roentgenol 2000; 174:132-134.
Citations
Citations to this article as recorded by