중심단어
TIPS, Left hepatic vein, Sonographic guidance,Transhepatic puncture
한글 초록
알코올성 만성 간염으로 인한 난치성 복수의 조절을 위해 경경정맥 간문맥-간정맥 단락술을 시행하였다. 우간엽의 심한 위축으로 좌간정맥을 통해 단락술을 시행했으며, 경정맥을 통한 좌간정맥의 선택이 어려워 초음파 유도하에 경피적 경로를 통해서 좌측 간문맥과 좌간정맥을 연이어 천자하는 기술을 이용하여 단락술을 시행하였다. 문맥-체정맥 압력차는 단락술 시행 후 49mmHg에서 27 mmHg로 감소하였다. 본 증례는 좌간정맥을 통한 경경정맥 간문맥-간정맥 단락술을 시행해야 하고 경정맥을 통한 접근만으로는 좌간정맥의 선택이 어려운 경우에, 초음파 유도하 경피적 경간으로 좌측 간문맥 및 좌간정맥을 연속적으로 천자하는 기술을 이용한 단락술의 시술이 가능한 대안임을 보여준다.
영문 초록
Transjugular intrahepatic portosystemic shunt(TIPS) was performed in a patient with chronic alcoholic hepatitis to control refractory ascites. TIPS was created between the left hepatic vein and left portal vein due to severe shrinkage of right lobe of the liver. Technique of ultrasound-guided percutaneous access into left portal vein and left hepatic vein in a single needle pass was utilized to place a TIPS since the selection of left hepatic vein via transjugular access was unsuccessful due to anatomical distortion of the liver. The portosystemic pressure gradient was reduced from 49 mmHg to 27 mmHg after TIPS formation. This case shows that the technique of serial transhepatic puncture of left portal vein and left hepatic vein under ultrasound guidance is a potential viable option when TIPS should be performed via left hepatic vein and its catheterization is unsuccessful.
Introduction
경경정맥 간문맥-간정맥 단락술을 시행하기 위해서, 보통 우측 간정맥으로부터 우측 간문맥으로 단락술을 시행하게 된다. 그 이유는 우간정맥의 직경이 크고, 우측 문맥과 가까우며 일정하게 문맥의 상후방에 위치하여, 우간정맥에서 우측문맥을 천자하기 쉽기 때문이다(1). 드문 경우에 중간정맥이나, 좌간정맥을 이용하게 되는데, 우간정맥이 막혀있거나 우간절제술을 받은 환자에서 중간간정맥이나 좌간정맥을 이용한 TIPS를 시행한 보고들이 있다 (2, 3). 그러나 좌간정맥의 선택이나, 좌간정맥에서 좌측 문맥을 천자하기 어려운 경우가 종종 있는데, 본고에서는 경피경간으로 좌측 간문맥의 분지와 좌간정맥을 한개의 바늘로 연속적으로 천자하여 TIPS를 시행한 예를 보고하고자 한다.
Case report
증례
70세 / 남자
임상소견
알콜성 간염을 앓고 있는 환자가 외부병원에서 추적 관찰중, 난치성 복수를 주소로 내원하였다. 환자는 복수 천자 및 이뇨제로도 복수가 조절되지 않아, 본과로 경경정맥 간문맥-간정맥 단락술 (TIPS)을 위해 의뢰되었다. 당시 환자는 Lasix 60mg을 bid로 복용하고 있었으며, daily 4L의 복수가 배액되고 있었다.
진단명
Alcoholic liver cirrhosis with refractory ascites
영상소견
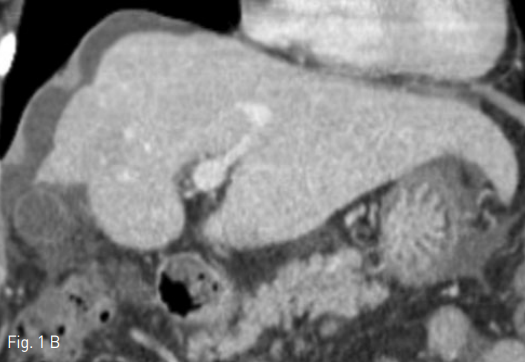
외부병원에서 시행한 컴퓨터 단층촬영(CT)검사에서, 간의 우엽은 심하게 위축되어 있었고 좌측외엽 및 미상엽은 증대되어 있어 만성간염에 합당한 소견이었다(Fig. 1). 이로 인하여 우측 간문맥 역시 매우 위축되어 있었으며, 우간정맥과 우측 간문맥의 거리가 멀어보였다.
시술방법 및 재료
시술을 위해, 우선 초음파 유도하에 우측 내경정맥을 천자한 후, Ring transjugular intrahepatic access set (Cook, Bloomington, IN, USA)내의9-Fr sheath (Cook, Bloomington, IN, USA )를 삽입하였고, 우측 총대퇴동맥을 천자하여 5-Fr vascular sheath (Terumo, Tokyo, Japan)를 삽입하였다. 5-Fr RH catheter (Cook, Bloomington, IN, USA) 를 이용하여 상장간동맥을 선택하여 간접문맥 조영술을 시행하였을 때, CT 소견과 마찬가지로, 우측 간문맥의 크기가 매우 작아져 있어 우간정맥에서 간문맥을 천자하기가 어려워 보였다 (Fig. 2). 이에 따라서, 좌간정맥으로부터 좌측간문맥으로의 단락을 만들기로 계획하였다. 우측 내경정맥의 9-Fr sheath를 통해, 5-Fr multipurpose catheter(Cook, Bloomington, IN, USA) 및 0.035-inch guide wire를 삽입하여 좌간정맥의 선택을 시도하였으나 실패하였다. 이에, 경피경간으로 좌측 간문맥과 좌간정맥을 연이어 천자하는 방법을 시도하기로 하였다. 먼저, 시술전 시행한 CT영상으로 3차원 재구성 영상 기법을 이용하여, 좌측 간문맥을 초음파 유도하에 천자할 때와 유사한 사위축상면 영상을 재현했다 (Fig. 3). 이 영상을 참고로 하여 초음파 유도하에 21 Gauge Chiba needle로 좌측 간문맥의 3번 구역지를 천자하였다. 간문맥이 천자된 것을 소량의 조영제로 확인후, 바늘을 조금 더 전진시켜 좌간정맥을 천자하는데 성공하였다. 이후, 0.035-inch guide wire를 우측무명정맥까지 진입 시킨 후, 우측 내경정맥에 있는 9-Fr sheath를 통해 snare catheter를 삽입하여 이 guidewire를 잡아 9-Fr sheath 로 꺼내는데 성공하였다 (Fig. 4). 이 guidewire를 이용하여 5-Fr DAVIS catheter (Cook, Bloomington, IN, USA) 를 좌측 간문맥을 지나 상간정맥까지 위치시키는데 성공하였다 (Fig. 5). 이때 측정한 문맥체정맥 압력차는 49 mmHg였었다. 0.035-inch guide wire를 Amplatz Super Stiff Guidewire (Boston Scientific, Boston, MA, USA)로 바꾼 후 , 8mmX4cm Mustang balloon catheter (Boston Scientific, Boston, MA, USA)을 이용하여 tract을 확장한 후, 10mmX5cm self-expandable stent (niti-s vascular stent, Taewoong, Korea)를 삽입하였다. 그 후 측정한 문맥체정맥 압력차는 27 mmHg로 감소하였으며, 시술 후 시행한 문맥조영술 상 간내문정맥 단락을 통한 흐름이 유지됨을 확인하였다 (Fig. 6). 좌측 간문맥의 3번 구역지를 천자했던 경로를 3mm × 3cm MReye Embolization Coil (Cook, Bloomington, IN, USA) 과 histoacryl과 lipiodol을 1:5로 혼합한emulsion을 이용하여 색전하고 시술을 종료하였다.
Fig 1A
Contrast enhanced CT scan showed features of chronic liver disease. Axial (A) and coronal (B) images showed hypertrophy of caudate lobe and lateral segments of left lobe with concomitant severe atrophy of the right lobe.
Fig 1B
Contrast enhanced CT scan showed features of chronic liver disease. Axial (A) and coronal (B) images showed hypertrophy of caudate lobe and lateral segments of left lobe with concomitant severe atrophy of the right lobe.
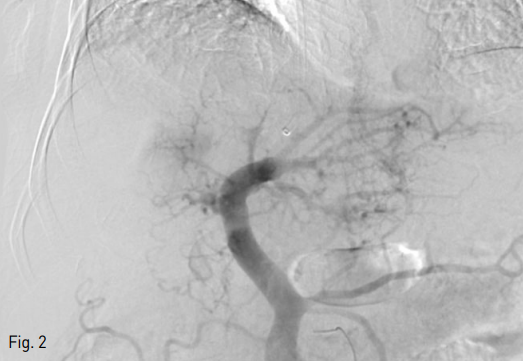
Fig 2
Indirect portography was obtained during the venous phase following iodinated contrast medium injections in the superior mesenteric artery (SMA). Digital subtraction image of portography showed that the diameter of the right portal vein was much smaller than that of the left portal vein.
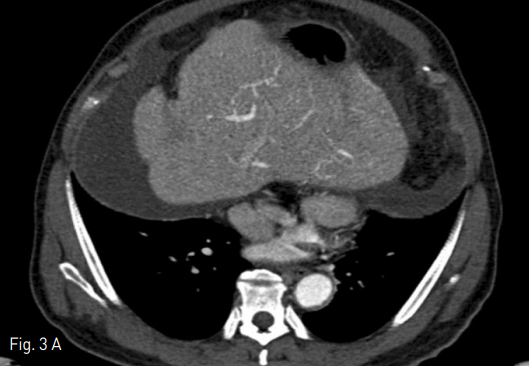
Fig 3A
Oblique axial plane was reconstructed (A) before performing procedure to facilitate sonographic guidance to puncture the left portal vein and left hepatic vein (B).
Fig 3B
Oblique axial plane was reconstructed (A) before performing procedure to facilitate sonographic guidance to puncture the left portal vein and left hepatic vein (B).
Fig 4A
Intraportal entry was confirmed by contrast injection on fluoroscopy (A).
Fig 4B
Under sonographic and fluoroscopic guidance, the needle was advanced into the left hepatic vein (B).
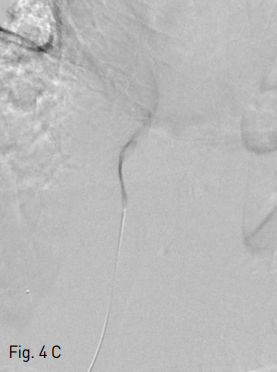
Fig 4C
Position of the needle into the left hepatic vein was confirmed by contrast injection (C).
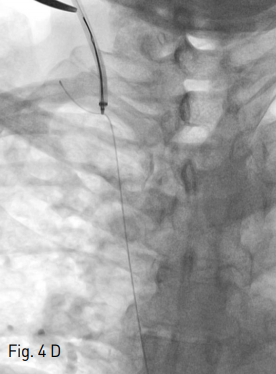
Fig 4D
A 0.035-inch guidewire was passed through the left hepatic vein, IVC, right atrium and SVC into the right innominate vein. Then transhepatic wire was snared using snare catheter providing through-and-through access (D).
Fig 5A
A 5-Fr Davis catheter was advanced over the guidewire to the left portal vein, then a small amount of contrast material was injected through 5-Fr catheter to see the location of the left portal vein (A).
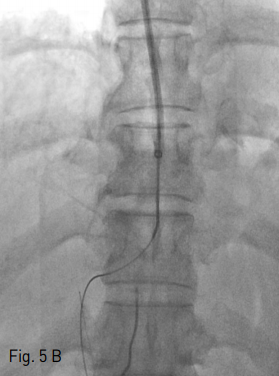
Fig 5B
After which, guidewire was introduced through the transjugular sheath and manipulated into the main portal vein and then superior mesenteric vein (B).
Fig 6
Final portography showed successfully established shunt tract via left portal vein.
고찰
경경정맥 간문맥-간정맥 단락술 시행시, 대부분의 경우에 전통적인 방법으로 우간정맥이나 중간정맥을 통해 시행할 수 있으며, 기술적 성공률은 93%이상으로 알려져 있다(4). 그러나 때에 따라서는, 좌간정맥을 통해 시술을 진행해야 할 경우가 있다. 우간정맥과 중간정맥이 우간엽절제술로 존재하지 않거나, 버드키아리 증후군 환자에서 우간정맥과 중간정맥이 혈전으로 막혀 있거나, 우간정맥이나 중간정맥이 비전형적인 해부학적 구조를 가져서 우측 간문맥보다 낮은 위치에 있는 경우가 그러한 경우이다. 본 증례는 만성간염으로 인하여 우측 간엽이 위축되어 있어서 우측 간문맥이 직경이 작고 우측 간정맥으로부터의 거리가 멀어 천자가 어려웠던 경우로, 좌간정맥을 통해 단락술을 시행하는 것이 대안이었었던 경우이다. 경경정맥 간문맥-간정맥 단락술 시행시, 간문맥을 천자하는 단계가 기술적으로 어려울 수 있는데, 천자횟수를 최소화하기 위해서 상장간동맥을 통한 간접 문맥 조영술, wedge 우간정맥 조영술, 초음파 유도하 천자, 자기공명 혈관촬영술 유도하 천자 등 여러 방법들이 고안되어 왔다(5, 6). 그러나 만성 간염이나 간경화로 인하여 간이 위축되고, 간의 해부학적 구조가 심하게 뒤틀린 환자의 경우, 간 내에서의 간정맥과 간문맥의 위치 변화로 인하여 전통적인 방법으로는 간문맥 천자가 어렵거나 또는 간정맥의 선택이 어려울 수 있다. 이러한 경우, 초음파 유도하에 경피적 경간 접근으로 간문맥 천자후 연속해서 간정맥을 천자하여 단락술을 시행할 수 있다(7, 8). 본 증례는, 좌간정맥을 이용한 간문맥-간정맥 단락술의 기술적 성공 사례를 보여주고 있으며, 우간정맥이나 중간정맥을 이용한 단락술이 어려울 경우 좌간정맥을 통한 단락술이 대안이 될 수 있음을 보여준다. 또한 경정맥을 통한 좌간정맥의 선택이 실패할 경우나 좌간정맥에서 좌측 문맥으로의 천자가 어려운 경우, 초음파 유도하에 경피적 경간으로 좌측 간문맥의 분지와 좌간정맥을 연이어 천자하여 단락술을 시행하는 것이 기술적으로 가능함을 보여주었다.
참고문헌
1. Uflacker R, Reichert P, D'Albuquerque LC, de Oliveira e Silva A. Liver anatomy applied to the placement of transjugular intrahepatic portosystemic shunts.
Radiology. 1994;191:705-712.
2. Hidajat N, Kreuschner M, Rottgen R, Schroder RJ, Schmidt S, Felix R. Placement of transjugular intrahepatic portosystemic shunt via the left hepatic vein under sonographic guidance in a patient with right hemihepatectomy. Acta Radiol 2003;44:363-365
3. Ganger DR, Klapman JB, McDonald V, et al. Transjugular intrahepatic portosystemic shunt (TIPS) for Budd-Chiari syndrome or portal vein thrombosis: review of indications and problems. Am J Gastroenterol. 1999;94:603-608
4. Tesdal IK, Jaschke W, Buhler M, et al. Transjugular intrahepatic portosystemic shunting (TIPS) with balloon-expandable and self-expanding stents: technical and clinical aspects after 3 1/2 years' experience. Cardiovasc Intervent Radiol 1997;20:29-37
5. Roizental M, Kane RA, Takahashi J, et al. Portal vein: US-guided localization prior to transjugular intrahepatic portosystemic shunt placement. Radiology. 1995;196:868-870
6. Kee ST, Ganguly A, Daniel BL, et al. MR-guided transjugular intrahepatic portosystemic shunt creation with use of a hybrid radiography/MR system. J Vasc
Interv Radiol 2005;16:227-234
7. Raza SA, Walser E, Hernandez A, Chen K, Marroquin S. Transhepatic puncture of portal and hepatic veins for TIPS using a single-needle pass under sonographic
guidance. AJR Am J Roentgenol 2006;187:W87-91
8. Liang HL, Liu WC, Huang JS, et al. TIPS in patients with cranial porta hepatis: ultrasound-guided transhepatic portohepatic-portocaval puncture in single needle pass. AJR Am J Roentgenol 2011;196:914-918
Citations
Citations to this article as recorded by