중심단어
Bronchobiliary fistula, bronchial embolization
한글 초록
기존 방식으로 치료가 어려웠던 기관지담관누공에 대하여 중재적 시술을 통해 성공적으로 치료하였던 증례를 보고하고자 한다. 환자는 간농양에 동반된 기관지 담관누공으로 2주간의 피부경유배액술 치료에도 증상이 호전되지 않았다. 이에 투시유도 하에 기존 피부경유배액술 경로를 이용하여 microwire와 microcatheter로 선택적으로 누공과 연결된 기관지까지 통과하였고, 누공과 연결된 기관지에 플러그를 연속적으로 설치하여 누공을 폐쇄하였다. 이후 추적 관찰에서 누공이 폐쇄되었고 환자의 증상이 소실되었다.
영문 초록
In this report, we herein report a successful case of treating intractable bronchobiliary fistula with interventional procedure. The patient had suffered from hepatic abscess with bronchobiliary fistula and there was no symptom improvement during more than two weeks despite of percutaneous drainage treatment. Under fluoroscopic guidance, we used percutaneous drainage tube as an access route. Then we selected fistula tract with microwire and catheter, embolized bronchus directly communicated with fistulas using tandem arrayed vascular plugs. After procedure, bronchobiliary fistula was occluded and symptom disappeared.
Introduction
기관지담관누공은 간 농양 또는 간의 암성 질환에 의하여 발생하는 드문 합병증이다. 담즙이 섞인 기침, 발열, 우상복부 및 우측 흉부 통증이 주된 증상이다. 내시경적 또는 경피적으로 배액관을 설치하여 누공이 막히기를 기대하는 것이 일반적인 치료방법이고 수술적 치 료가 가장 마지막에 고려되는 치료방법이나, 이러한 치료에 잘 반응하지 않는 경우 2차 치료가 어렵고 적절한 시기에 치료가 되지 않을 경우 반복적인 폐렴을 유발하여 치명적인 결과를 유발하기도 한다. 본 증례에서는 간내담관암의 횡격막 침범 및 농양 형성에 의하여 발생한 난치성 기관지담관 누공에 대하여 경피적으로 접근하여 혈관 플러그를 누공과 연결된 기관지에 연속적으로 설치하여 성공적으로 치료한 경험을 보고하고 잘한다.
Case report
증례
64세/여자
임상소견
환자는 간내담관암으로 간우엽절제술 및 미상엽 절제술을 받았다. 절제 부위 (resection margin) 재발 및 장관문합부위 침범으로 인한 폐쇄성 황달이 발생하여 PTBD를 시행 받았다. 이후 발열과 담즙성 기침 (biliptysis) 이 발생하였다. 항생제 사용 후 발열은 감소하였으나 bilitypsis는 점차 악화되어 심한 호흡곤란을 호소하였다.
진단명
Bronchobiliary fistula due to tumor invasion at the right diaphragmatic area
영상소견
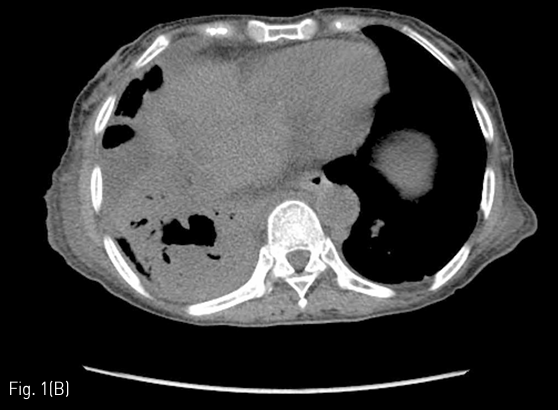
전산화 단층촬영에서 간우엽절제부-장문합부에 재발암의 침범이 있으며 이 병변이 우측 횡격막 및 폐실질을 침범하고 이와 동반된 폐농양이 폐우하엽에 보였다 (Fig. 1A-B).
시술방법 및 재료
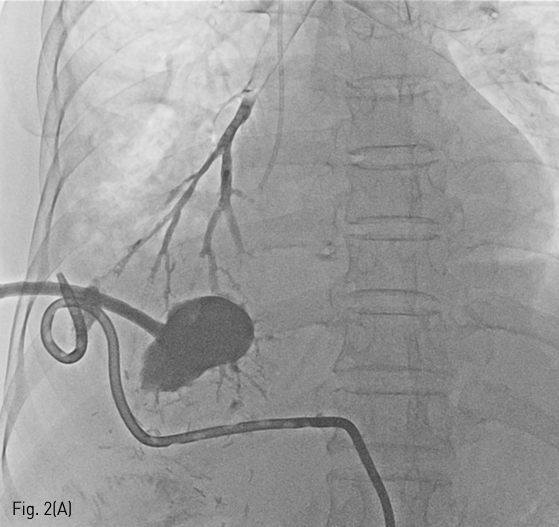
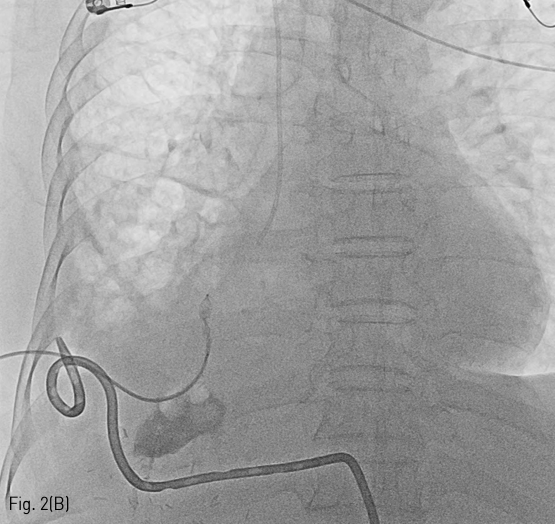
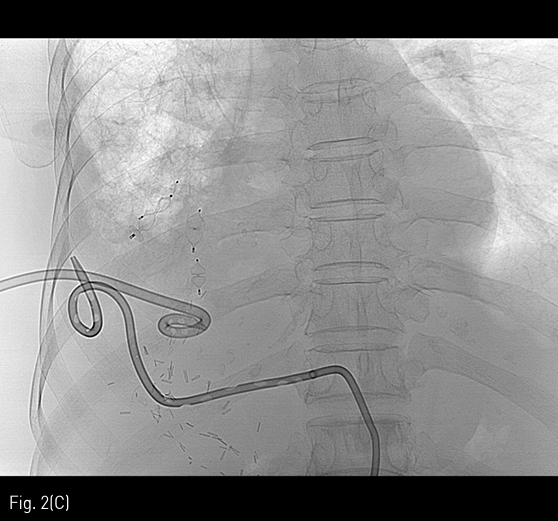
Lung abscess에 대하여 transthoracic approach로 12Fr pigtail catheter를 삽입하여 내용물을 배액하였다. 경과 관찰 중에도 biliptysis가 지속되고 기침이 점차 악화되는 소견이 보여 PCD tube로 contrast를 주입하고 tubogram 시행하였을 때 cavity와 연결된 가느다란 여러 가지의 bronchus가 보였다 (Fig. 2A). 해당 가지들을 microcatheter (Progreat α, Terumo, Tokyo, Japan) 및 0.018 inch microwire (Meister, Asahi, Nagoya, Japan)을 써서 cannulation 하였고 5Fr catheter (Davis, Cook Inc, USA; omni, merit medical, Bloomington, USA)를 진입시킨 후 vascular plug type 4 8mm & 7mm (AMPLATZER, St.Jude medical, St. Paul, USA)를 이용하여 서로 겹치도록 나란히 위치시켜서 embolization을 시행하였다 (Fig. 2B-C). 이후 lung abscess에 위치시킨 pigtail catheter는 합병증 없이 제거하였다.
추적관찰
시술 후 biliptysis는 완전히 소실되었고 그에 따른 기침 및 호흡곤란 역시 소실되었다.
Fig 1A
64-year-old woman with fever, biliptysis and dyspnea. An axial CT scan shows recurred tumor along resection margin of left lobe of liver and dilated bile ducts (A), and a lung abscess in right lower lobe (B).
Fig 1B
64-year-old woman with fever, biliptysis and dyspnea. An axial CT scan shows recurred tumor along resection margin of left lobe of liver and dilated bile ducts (A), and a lung abscess in right lower lobe (B).
Fig 2A
A radiographic image after injection of contrast via PCD tube to lung abscess, shows direct communication to bronchus of right lower lobe (A).
Fig 2B
A radiographic image of embolization of communicated bronchus using vascular plug (B).
Fig 2C
Image obtained after completion of bronchus embolization (C).
고찰
Bronchobiliary fistula는 드물지만 치명적이고 치료에 잘 반응하지 않는 질환으로 알려져 있다. 간 농양 내지 폐농양에 병발하는 경우가 흔하고, 우상복부 및 우측 흉통 및 담즙이 섞인 기침이 주된 증상이며 객담 내 bilirubin 농도를 측정하는 것이 진단에 도움을 줄 수 있다.
일반적인 치료 방법은 경피적 또는 내시경적으로 배액술을 시행하는 것이다. 2주 이상의 치료에도 호전되지 않는 경우 병변이 위치하는 간엽 또는 폐엽 절제술, 누공 절제술과 같은 수술적인 치료가 요구되나 수술자체에 따른 위험이 따르고 환자가 수술을 견딜 수 없는 상태인 경우도 흔하다.
본 증례의 경우에 담관암으로 인한 간우엽전절제술 후 절제 부위에서 재발한 종양의 침범으로 횡격막 및 폐의 직접 침범 및 폐농양이 발생하여 intractable bronchobiliary fistula가 초래되었으며 투시하에 농양과 연결성을 보이는 기관지 자체를 vascular plug로 embolization 하여 좋은 효과를 보였던 경우이다.
본 시술과 같은 방식의 치료를 기존 문헌고찰로는 발견하기가 어려웠다. 그러나 끈적끈적한 담즙은 vascular plug의 세밀한 strut 사이를 통과하기가 어렵고 plug 자체가 압력 변화가 심한 흉강 내에서 물리적 지지력을 가지며 효과적으로 담즙의 역류를 차단할 수 있을 것으로 기대되었다. 시술 후 biliptysis가 완전히 소실되고 그에 따른 기침 및 호흡곤란도 없어져 임상적인 증상 개선을 얻을 수 있었다. 그러나, 기관지를 막는 시술이므로 이론적으로는 색전한 기관지의 원위부에 폐허탈 (atelectasis) 내지 폐렴이 초래될 수 있다. 본 증례에서는 색전된 기관지의 원위부가 종양의 직접 침범 및 농양 형성에 의한 실질 파괴로 거의 남아 있지 않아 위에 언급한 합병증이 발생하지는 않은 것으로 추정된다.
참고문헌
1. Chua HK, Allen MS, Deschamps C, Miller DL, Pairolero PC. Bronchobiliary fistula: principles of management. Ann Thorac Surg 2000;70:1392-1394.
2. Eryigit H, Oztas S, Urek S, Olgac G, Kurutepe M, Kutlu CA. Management of acquired bronchobiliary fistula: 3 case reports and a literature review. J Cardiothorac Surg 2007;2:52
3. Kim KH, Lee KH, Won JY, Lee DY, Paik HC, Lee DY. Bronchopleural fistula treatment with use of a bronchial stent-graft occluder. J Vasc Interv Radiol 2006;17:1539-1543
4. Liao GQ, Wang H, Zhu GY, Zhu KB, Lv FX, Tai S. Management of acquired bronchobiliary fistula: A systematic literature review of 68 cases published in 30 years. World J of Gastroenterol 2011;17:3842-3849.
5. Mandal A, Sen S, Baig SJ. Bronchobiliary fistula. J Minim Access Surg 2008;4:111-113
Citations
Citations to this article as recorded by