중심단어
Splenic arterial embolization, splenomegaly, severe thrombocytopenia
한글 초록
간경화가 있는 57세 여자 환자가 수혈에 반응하지 않고 지속되는 심한 혈소판 감소증이 있어 이에 대한 치료를위해 색전술이 의뢰되었다. 비장동맥의 middle segmental branch를 보존하며 superior, inferior segmental branches를detachable coils, gelfoam, N-butyl-cyanoacrylate을 사용하여 색전하였고 비장의 일부 실질을 제외하고 경색을 유도하였다. 치료 2주 후부터 혈소판 수치가 정상범위 내로 회복되어 유지되고 있다.
영문 초록
A 57-year-old woman with liver cirrhosis suffered from severe thrombocytopenia which is intractable despite transfusion. For this reason, she was referred to our department for embolization. While preserving the middle segmental branch of splenic artery, superior and inferior branches were embolized using detachable coils, Gelfoam, and N-butyl cyanoacrylate. Embolization induced splenic infarction except small portion of the splenic parenchyma. Platelet count was restored to the normal range after two weeks and has been maintaining thereafter.
Introduction
비장동맥 색전술은 인터벤션 영상의학분야에서 점점 더 흔해지고 있는 추세로, 외상에 의한 비장손상이나 비장기능항진증, 문맥고혈압, 비장동맥동맥류 및 가성동맥류에 대한 치료법으로 중요한 역할을 하고있다. 그 중에서 비장기능 항진증은 비장비대, 혈소판감소증, 백혈구감소증, 빈혈을 일으키는데 비장적출술은 이에 대한 치료에 있어 효과적이지만 인체의 면역기능 저하를 일으키기 때문에 성공적인 비장동맥 색전술이 그 대안이 되었다. 비장동맥 색전술을 시행하여 심한 혈소판 감소증을 성공적으로 치료하여 보고하고자 한다.
Case report
증례
57세/여자
임상소견
HBV와 관련된 간경화 환자로 비장비대로 인해 발생한 지속되는 심한 혈소판 감소증에 대한 교정을 위해 혈소판 수혈에도 효과가 없어 비장동맥 색전술이 의뢰 되었다.
진단명
Splenomegaly due to HBV-related liver cirrhosis
영상소견
간경화와 비장비대 및 esophageal, paraesophageal, and gastric fundal varices가 복부 전산화단층촬영에서 확인되었다(Fig. 1).
시술방법 및 재료
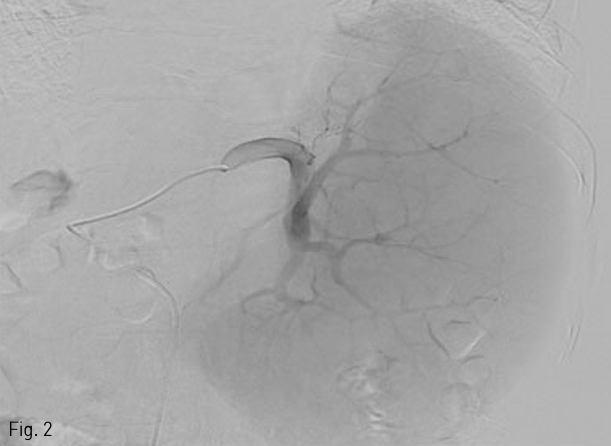
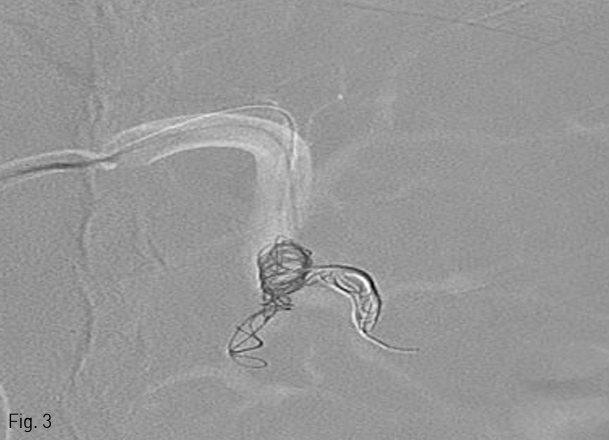
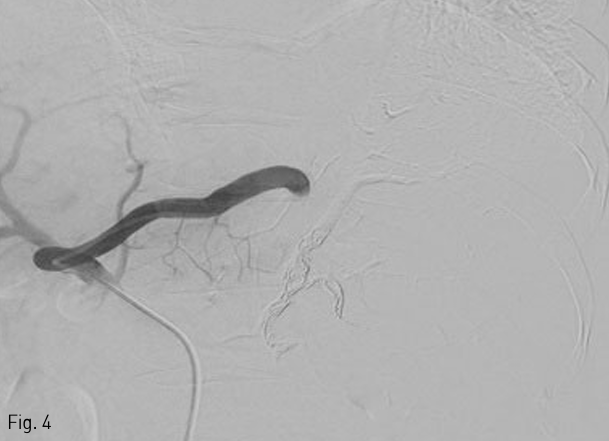
5 Fr Yashiro catheter (Terumo, Tokyo, Japan)를 복강동맥을 통해 비장동맥에 삽입한 후 혈관조영술을 시행하여 비장동맥의 분지들을 먼저 확인하였다 (Fig. 2). 0.021 inch guide wire (GT guide wire; Terumo)와 2.7 Fr microcatheter (Progreat; Terumo, Tokyo, Japan)를 이용하여 co-axial technique으로 middle segmental artery가 분지된 이후 splenic hilum에서의 비장동맥에 12mm×3cm 1개, 10mm×3cm 3개의 platinum coils (IDC: Interlocking Detachable Coil; Boston Scientific, Tokyo, Japan)와 gelfoam (Cutanplast, Mascia Brunelli Spa, Milano, Italy), N-butyl cyanoacrylate (NBCA; Histoacryl; B.Braun, Melsungen, Germany)와 Lipiodol (Guerbet, Paris, France) 1:4 혼합물을 이용하여 superior, inferior segmental artery를 색전하였다 (Fig. 3). 색전 후 비장동맥 조영술에서 splenic hilum level에서 원위부 색전이 이루어진 것을 확인하였다(Fig. 4).
추적관찰
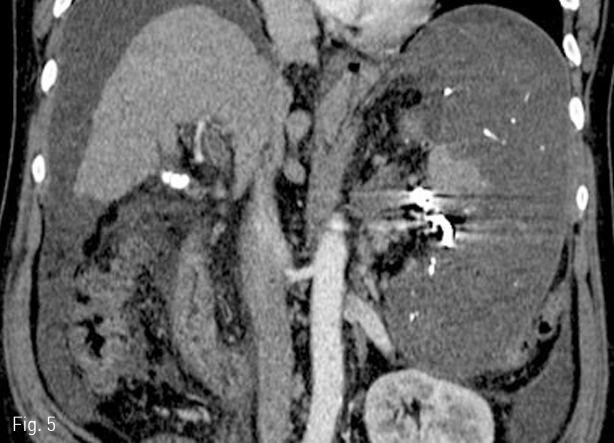
환자는 색전술 후 백혈구 수치가 상승하고 발열증상이 있었으나 보존적 치료 후 완전히 회복되었다. 1개월 뒤 시행한 복부 전산화 단층촬영에서 hilum주위의 일부 비장 실질을 제외한 비장의 대부분의 경색이 초래되었다 (Fig. 5). 색전술을 시행하고 2주 후에 혈소판 수치는 정상범위 내로 증가되었고 이후 12개월까지 유지되고 있다.
Fig 1
Arterial phase of abdominal CT scan shows liver cirrhosis with marked splenomegaly and gastric fundal varix.
Fig 2
Angiogram for splenic artery shows superior, middle, and inferior segmental branches.
Fig 3
Road map image shows deployment of several detachable coils into the inferior branches of splenic artery during embolization.
Fig 4
Completion angiogram demonstrates occlusion of the distal branches of splenic artery at the hilum.
Fig 5
Follow-up CT scan obtained 1 month after embolization shows splenic infarction except small portion of the splenic parenchyma.
고찰
비장의 소비적인 과활동성을 줄이기 위해 의도적인 비장경색을 유도하기 위해 1973년에 Maddison은 처음으로 비장동맥 색전술을 시행하였다. 하지만 complete splenic infarction으로 인한 심각한 합병증으로 인해 치료옵션으로 받아들여지지 못했다. 이후에 hematological response와 합병증의 심각한 정도는 경색된 비장조직의 양과 상관관계에 있는 것이 밝혀져 비장동맥 색전술을 시행할 때 과도한 비장경색을 피하는 partial splenic embolization이 시도되었다. 현재 많은 인터벤션 의사들은 비장기능 항진증의 치료를 위해 60-70%의 비장 경색을 목표로 색전술을 시행하고 있다. 그 중 한가지 방법은 비장동맥의 몇 개의 원위분지만을 선택적으로 막은 후 parenchymal phase angiogram을 얻어 남은 viable splenic tissues의 부피를 추정하고 색전이 부족할 경우 추가적으로 원위분지를 막아 60-70%정도의 비장 경색을 유도하는 것이다. 다른 방법은 색전을 위한 catheter tip을 주 비장동맥에서 조금 더 근위부에 위치시키되 major pancreatic branches를 지나도록 위치시키고 비선택적인 partial embolization을 시행하는 것이다. 이 때 parenchymal blush가 감소될 때까지 색전물질을 주입한다. 색전 물질로 가장 많이 사용되는 것은 gelatin sponge pledget과 polyvinyl alcohol particle이고, coil이 비장내 분지들에 삽입될 경우 치료효과가 매우 좋았다는 보고가 있다. 지금까지 여러 의료기관들에서 통일된 색전 방법은 없지만 ‘Spigos technique’으로 알려진 general guideline을 따른다면 합병증을 의미있게 줄일 수 있다. 이 프로토콜은 시술 전후에 광범위 항생제를 사용하고 색전물질과 항생제를 섞어 투여하며 80%이상의 과도한 색전을 피하는 것이다(1). 본 증례에서는 비장동맥의 middle segmental artery가 먼저 분지되어 나머지 segmental arteries만을 색전할 수 있어 비장의 일부를 보존할 수 있었던 경우였다. 환자는 시술 후 감염증상을 보였으나 심각한 합병증을 일으키지는 않았고 보존적 치료로 전신상태가 회복되었다. 또한 혈소판 수치도 한달 이내에 정상적으로 회복되었고 그 이후 유지되어 성공적인 치료 효과를 보였다. 목표로 하는 60-70%정도의 비장 경색을 유도하는 것이 쉽지는 않으나 첫번째 시술에서 무리하게 색전하지 않고 필요하다면 추가적인 시술로 목표로 하는 경색을 유도하는 단계적 색전술도 좋은 방안이 될 수 있을 것으로 판단된다.
참고문헌
1. Madoff DC, Denys A, Wallace MJ, et al. Splenic Arterial Interventions: Anatomy, Indications, Technical Considerations,and Potential Complications. Radiographics 2005;25:S191-211
2. Luz JH, Luz PM, Marchiori E, et al. Partial splenic embolization to permit continuation of systemic chemotherapy. Cancer Med 2016;5:2715-2720
3. Kumpe DA, Rumack CM, Pretorius DH, Stoecker TJ, Stellin GP. Partial splenic embolization in children with hypersplenism. Radiology 1985;155:357-362
4. Bessoud B, Denys A. Main splenic artery embolization using coils in blunt splenic injuries: effects on the intrasplenic blood pressure. Eur Radiol 2004;14:1718 1719
Citations
Citations to this article as recorded by