중심단어
Balloon Venoplasty, Budd-Chiari Syndrome, Membranous Obstruction of the Vena Cava
국문 초록
Budd-Chiari Syndrome (BCS)은 hepatic venous outflow의 일부 또는 완전 폐색에 의한 흔치 않은 질환이다. 증상의 중증도에 따라 다양한 치료법이 사용될 수 있다. 본 증례는 하지 통증과 저림을 주소로 내원한 46 세 남자 BCS 환자에서 double balloon technique을 이용하여 성공적으로 치료한 1예를 보고하고자 한다.
영문 초록
Budd-Chiari Syndrome (BCS) is a rare disease caused by partial or complete obstruction of hepatic venous outflow tract. Depending on the disease severity, various management strategies have been proposed. In this case report, we present a case of successful venoplasty using double balloon technique for a 46-year-old BCS patient with both leg pain and numbness.
Introduction
Budd-Chiari Syndrome (BCS)은 hepatic venous outflow의 일부 또는 완전 폐색을 보이는 질환으로 이 폐색은 작은 간정맥부터 하대정맥과 우심방까지 발생할 수 있다. 주로 간정맥에 발생하는 서양권 BCS 환자들과 달리 동양권 환자들의 경우 보통 inferior vena cava (IVC) occlusion의 형태로 발견된다 (1). 다양한 원인이 있을 수 있는데 특발성이 가장 많으며 혈전, membranous webs 등이 원인으로 알려져 있다. 임상 양상은 다양하여 증상이 없을 수도 있지만 적절한 치료가 없을 경우 급성 또는 만성 간질환이 발생할 수 있다. 본 고에서는 하지 통증과 저림 증상으로 내원한 BCS 환자에서 double balloon technique을 적용한 증례를 소개하고자 한다.
Case report
증례
46세/남자
임상소견
원인 불명의 간경화 환자로 내원 2년 전부터 오래 걸을 때 발생하는 하지 통증과 저림 증상 발생하였으며 타 병원에서 촬영한 lumbar MRI에서 spinal dural arteriovenous fistula 의심되어 내원하였다. 내원하여 촬영한 spinal angiography에서 특이 소견 없어 촬영한 복부 CT에서 membranous obstruction of the inferior vena cava (MOVC) with Budd�Chiari syndrome 가 확인되어 venoplasty 가 의뢰되었다.
진단명
Membranous obstruction of the inferior vena cava (MOVC) with Budd-Chiari syndrome
영상소견
원인 불명의 간경화 환자로 내원 2년 전부터 오래 걸을 때 발생하는 하지 통증과 저림 증상 발생하였으며 타 병원에서 촬영한 lumbar MRI에서 spinal dural arteriovenous fistula 의심되어 내원하였다. 내원하여 촬영한 spinal angiography에서 특이 소견 없어 촬영한 복부 CT에서 membranous obstruction of the inferior vena cava (MOVC) with Budd�Chiari syndrome 가 확인되어 venoplasty 가 의뢰되었다.
시술방법 및 재료
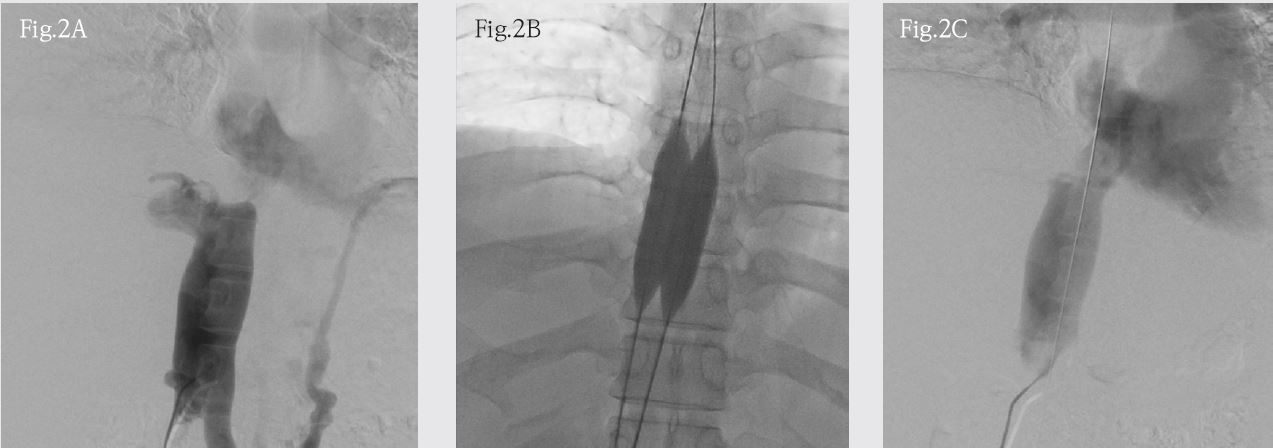
환자의 right common femoral vein을 초음파 유도 하에 천자한 후 7-F sheath를 삽입하였다. 0.035-inch, 180 cm long hydrophilic guide wire (Radiofocus Giude Wire M: Terumo, Tokyo, Japan) 와 5-F Headhunter catheter (Cook, Bloomington, IN)를 IVC에 위치시키고 venogram을 얻었다 (Fig. 2A). 이후 wire를 좁아져 있는 inferior vena cava (IVC)로 통과시켰다. 새롭게 right common femoral vein을 같은 방식으로 한번 더 천자한 후 새로운 wire를 IVC로 통과시켰다. 두 wire를 260 cm Lunderquist wire (Cook, Bloomington, IN) 로 교체한 이후 14 mm sized balloon catheter (XXL balloon dilatation catheter: Boston scientific, Natric, MA)를 이용하여 좁아져 있는 IVC에 balloon dilatation을 시행하였고 순차적으로 추가로 같은 balloon catheter 한 개를 더 사용하여 double balloon dilatation을 시행하였다 (Fig. 2B). Balloon catheter를 제거한 이 후 Headhunter catheter를 이용하여 completion venography를 시행하고 시술을 완료하였다 (Fig. 2C).
추적관찰
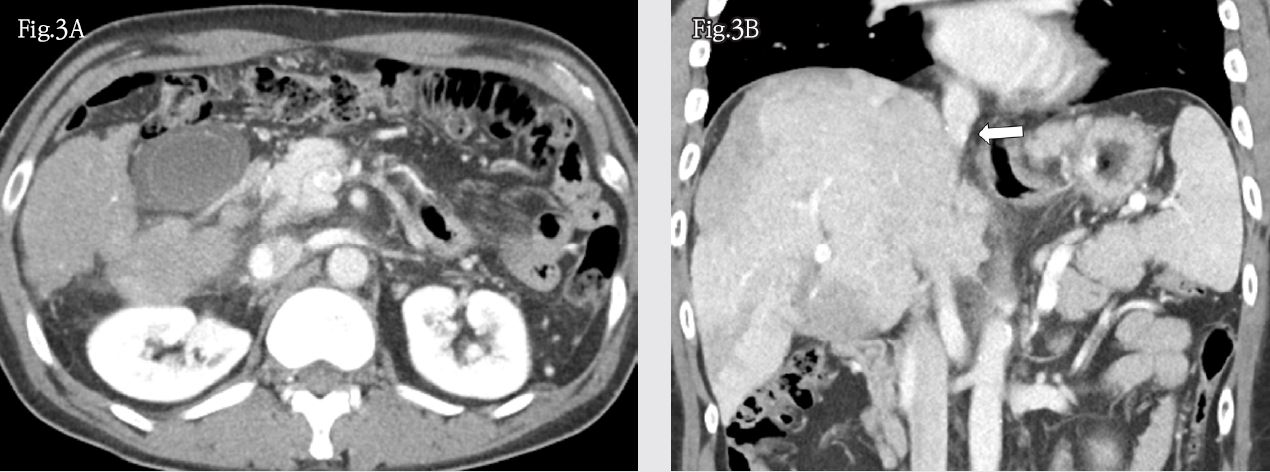
시술 후 합병증 없었으며 증상은 호전되었다. 약 15 개월 후 외래 경과 관찰 하면서 시행한 abdomen CT에서 liver cirrhosis 소견은 지속되었으나 간 실질은 homogenous enhancement를 보였으며 IVC의 septum-like structure와 collateral flow는 사라졌음을 확인하였다 (Fig. 3A, 3B).
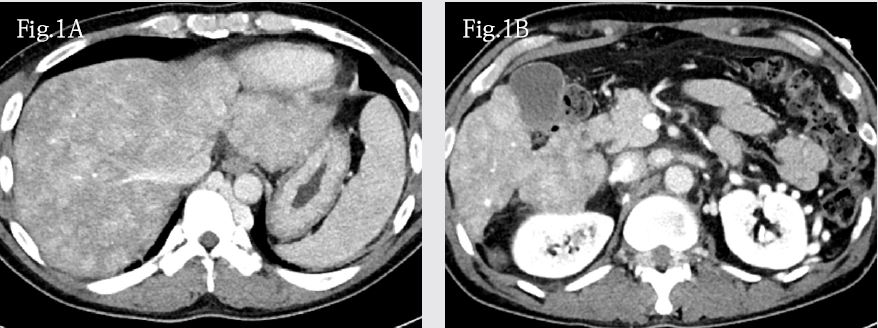
Fig. 1. A, B
Fig. 1. (A, B) Contrast-enhanced axial CT image shows liver cirrhosis with heterogenous enhancement of liver parenchyma. Middle and left hepatic veins are invisible on CT scan. Prominent azygous and hemiazygous veins are noted. Also, both epigastric veins, lumbar veins and epidural venous plexus are prominent.
Fig. 1. C
(C) Thoracic spine axial MR image shows dilated epidural veins around the spinal cord (arrow).
Fig. 1. D
(D) On contrast-enhanced coronal CT image, arrow indicates septum-like structure within IVC.
Fig. 2. A, B, C
Fig. 2. (A) IVC venogram shows nearly complete occlusion of hepatic segment of IVC with collateral venous flow. (B) Double balloon venoplasty is performed using two XXL Balloon. (C) Completion venogram shows patent IVC with disappeared collateral venous flow.
Fig. 3. A, B
Fig. 3. (A) Contrast-enhanced axial CT image shows disappearance of engorged epidural venous plexus and other collateral veins. (B) Contrast-enhanced coronal CT image shows patent IVC without septum-like structure (arrow)
고찰
BCS는 다양한 임상 양상으로 발견될 수 있다. 본 증례의 환자처럼 chronic BCS 가 liver cirrhosis를 야기할 수 있다. 또한 radiculopathy 또는 myelopathy 증상으로 나타날 수 있다. 한 연구에서 9640명의 back pain 또는 sciatica 환자를 살펴보았을 때 0.13%인 13명에서 IVC occlusion이 원인이었다고 보고한 바 있다 (2). 이는 IVC outflow obstruction에 의한 venous hypertension이 epidural venous congestion을 만들고 척수의 arteriovenous pressure gradient를 감소시켜 tissue perfusion 감소에 의한 ischemia를 유발하기 때문이다 (1). 이전에 발표된 문헌들을 살펴보면 이 등의 case report에서 하지 근력 저하와 배뇨 장애를 보인 BCS 환자에서 IVC segmental occlusion에 Colapinto needle을 이용해 puncture 후 stent-graft를 삽입하여 환자 증상을 완치시켰다고 보고하였다 (3). Carvalho 등도 허리 통증과 하지 근력 저하를 보인 BCS 환자에서 IVC occlusion에 serial balloon dilatation과 stent insertion을 통하여 증상을 완치시켰다고 보고하였다 (4). MOVC에서 balloon dilatation은 높은 성공률을 보인다. 한 연구에서 MOVC의 balloon dilatation 후 8.9%의 낮은 재협착률을 보였으며 segmental occlusion 일 경우 재협착의 위험이 높아진다고 보고 하였다 (5). IVC venoplasty 시 작은 balloon (≤ 20mm)를 이용할 경우 큰 balloon (> 20mm)를 이용할 때보다 높은 재협착과 recoiling을 보이며 이로 인해 큰 직경의 balloon을 이용하는 게 일반적이다 (6). 하지만 본 증례처럼 double balloon technique을 이용하는 경우 single large balloon 보다 몇 가지 장점이 있다. 큰 balloon catheter 보다 작은 balloon catheter는 조작하기 쉬우며 혈관 천자 시 혈관의 손상을 적게 줄 수 있다. 또한 작은 balloon catheter는 더 큰 pressure를 가할 수 있고 작은 balloon catheter를 동시에 inflation 할 경우 single plane에 더 큰 pressure를 가할 수 있다. Dilatation procedure 중에 두 balloon catheter 사이의 residual lumen 사이로 blood flow가 지나갈 수 있는 것도 장점이다 (7). 본 증례에서 double balloon technique을 이용하여 balloon dilatation 후 비교적 충분한 IVC dilatation을 이뤄 냈으며 추가적인 stent 삽입 없이 성공적으로 시술을 종료할 수 있었다.
참고문헌
1. Meng X, Lv Y, Zhang B, He C, Guo W, Luo B, et al. Endovascular management of budd-chiari syndrome with inferior vena cava thrombosis: A 14-year single�center retrospective report of 55 patients. J Vasc Interv Radiol 2016;27:1592-1603
2. Paksoy Y, Gormus N. Epidural venous plexus enlargements presenting with radiculopathy and back pain in patients with inferior vena cava obstruction or occlusion. Spine (Phila Pa 1976) 2004;29:2419-2424
3. Lee JH, Song WJ, Kang KC. Myelopathy-mimicking symptoms of epidural venous engorgement and syringomyelia due to inferior vena cava stenosis at the thoracolumbar junction in a patient with budd�chiari syndrome. J Neurosurg Spine 2015;23:467-470
4. Carvalho DZ, Hughes JD, Liebo GB, Bendel EC, Bjarnason H, Klaas JP. Venous congestive myelopathy due to chronic inferior vena cava thrombosis treated with endovascular stenting: Case report and review of the literature. J Vasc Interv Neurol 2015;8:49-53
5. Huang Q, Shen B, Zhang Q, Xu H, Zu M, Gu Y, et al. Comparison of long-term outcomes of endovascular management for membranous and segmental inferior vena cava obstruction in patients with primary budd-chiari syndrome. Circ Cardiovasc Interv 2016;9:e003104
6. Ding PX, Han XW, Liu C, Ding JY, Lee EW. Inferior vena cava rupture caused by balloon angioplasty during the treatment of budd-chiari syndrome. Cardiovasc Intervent Radiol 2019;42:1398-1404
7. Mullins CE, Nihill MR, Vick GW, 3rd, Ludomirsky A, O’Laughlin MP, Bricker JT et al. Double balloon technique for dilation of valvular or vessel stenosis in congenital and acquired heart disease. J Am Coll Cardiol 1987;10:107-114
Citations
Citations to this article as recorded by