중심단어
Pancreaticoduodenectomy, Pancreaticojejunostomy(PJ) catheter Migration, Intrahepatic stones, Percutaneous Transhepatic Removal.
국문 초록
췌십이지장절제술 이후 가장 치명적인 합병증인 췌공장문합부의 이자액 누출을 방지하기 위해 trans�anastomotic silastic stent 삽입하여 배액 하는 방법이 흔히 사용된다 이러한 trans-anastomotic silastic tent 의 위치 변경 및 이동 시 이자액의 누출로 인한 췌장루 및 카테터의 자극으로 인한 담관염 및 담석을 포함한 다양한 합병증이 나타날 수 있어 신속한 회수가 시행되어야 한다. 본 기고에서는 73세 남자 환자가 바터팽대부암으로 췌십이지장절제술 췌공장문합부에 삽입된 스텐트가 왼쪽 간내 담관으로 이동되어 있으며 담석이 관찰되어 경피경간경로를 통해 스텐트 및 담석 제거술을 시행한 증례이다.
영문 초록
Insertion of catheter at the pancreticojejunostomy (PJ) site after pancreatoduodenectomy (PD) is a common method to prevent critical complications such as pancreatic juice leakage. Malpositioning of the device may result in the impairment of proper drainage and persistent provocation of adjacent organs, leading to complications such as pancreatic fistula, cholangitis and intraductal stones. Thus, prompt removal of the migrated catheter must be carried out. We report a case of 73-year-old man with a migrated trans-anastomotic silastic stent from pancreaticojejunostomy site into the intrahepatic bile duct after PPPD, which was successfully removed through the percutaneous transhepatic approach using a snare.
Introduction
췌십이지장절제술은 팽대부 주위의 악성 또는 양성 종양에서 행해지는 외과적 절제술이다 (1-2). 췌공장문합부와 담관공장문합부를 통한 이자액 및 담즙 누출 등의 수술 후 합병증을 방지하기 위해 카테터를 삽입하여 배액 할 수 있다 (3). 하지만 이러한 기구 중 silastic stent는 특히 유연하고 호흡에 영향을 많이 받기 때문에 간내 담관으로 이동되기 쉽고 그 결과로 췌장루, 간농양, 담관염, 담관의 협착, 담석 등의 합병증이 나타날 수 있다 (4-8). 이동된 카테터는 내시경적 역행성 담관췌관 조영술(ERCP) 혹은 경피적 경로를 통해 제거 가능하다 (6-9). 하지만 수술 후 해부학적 구조가 변하여 내시경 이 접근하기 어려운 경우 경피경간경로를 통해 스텐트를 제거하는 것이 합병증을 예방하고 치료할 수 있는 유용한 해결책일 수 있다.
Case report
증례
73세/남자
임상소견
특별한 기저질환이 없던 환자로, 서서히 발생한 체중 감소로 본원에서 시행한 복부 컴퓨터단층촬영에서 샘창자까지 침범한 바터팽대부암으로 진단되었다. 환자는 췌십이지장절제술과 이자빈창자연결술 및 항암치료를 시행하였으며, 약 2년 후 시행한 추적 복부 컴퓨터단층촬영에서 간내 담석 및 담관 확장과 담관염 소견이 관찰되어 PTBD를 시행했다.
진단명
Intrahepatic catheter migration, Intrahepatic stones, Cholangitis.
영상소견
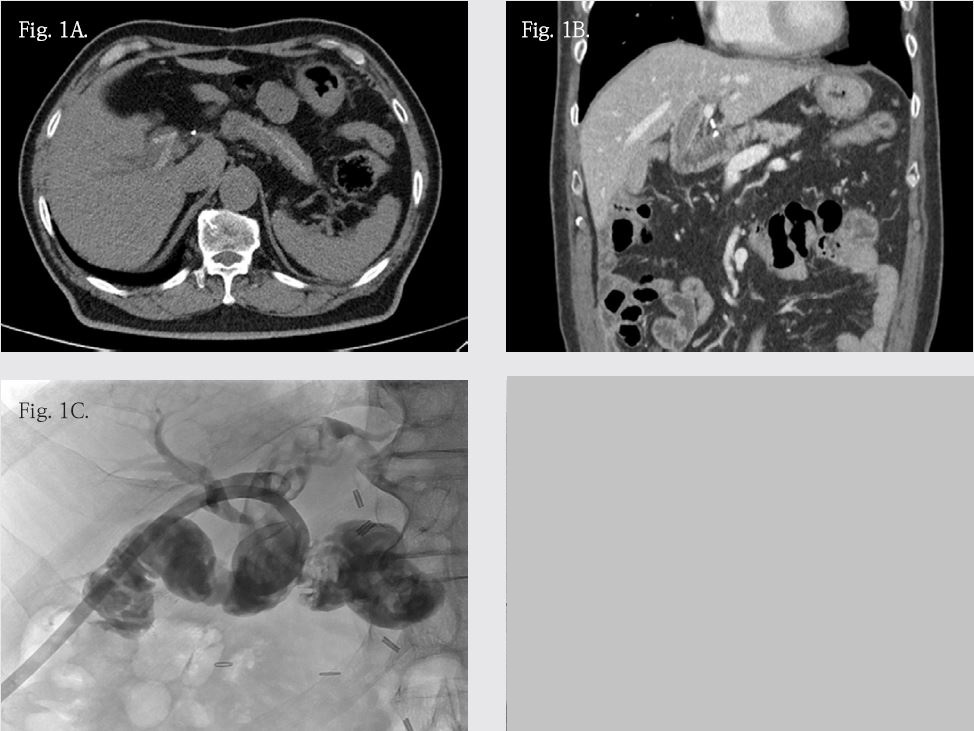
복부 컴퓨터단층촬영에서 수술 당시 췌공장문합을 시행한 위치에 협착을 예방하기 위해 삽입한 카테터가 왼쪽 간관으로 이동되어 있으며 양측 간관과 총담관에 담석이 관찰되고 담관 확장 및 담관염이 동반되어 있었다 (Fig. 1A, B). 카테터 위치 변경으로 인해 간내 담석이 발생한 것으로 의심되어 카테터 및 담석에 대한 경피경간 경로를 통한 제거술이 의뢰되었다.
시술방법 및 재료
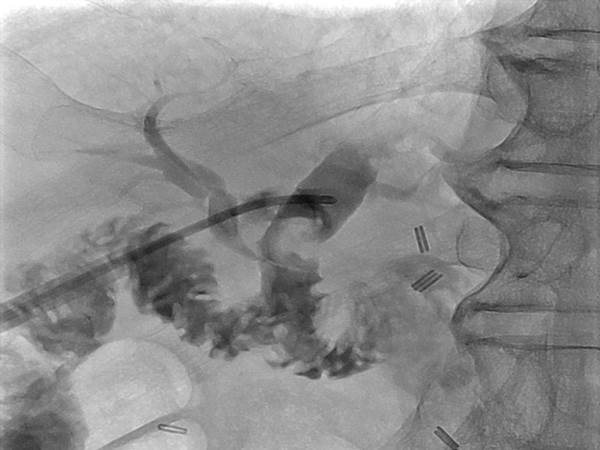
PTBD 시행 4일 후에 얻은 담관 조영술에서 다수의 담석들과 공장부터 왼쪽 간관까지 지렁이 모양의 충만 결손이 있었고, 이는 왼쪽 간내 담관으로 이동한 trans-anastomotic silastic stent로 추정되었다 (Fig. 1C). Fogarty balloon catheter (Edwards Lifesciences, CA, USA)를 결석의 뒤로 이동시켜 우측 후방 격벽성 담관 (right posterior septal duct) 및 왼쪽 간관에 있는 결석을 공장 안으로 밀어내는 결석 제거술을 시행했으며 12F drainage catheter (SungWon medical, Chung-Ju, Korea)를 삽입한 후 시술을 종료하였다. 이틀 뒤 PTBD catheter를 통해 14Fr sheath (Check Flo, Cook, IN, USA)를 삽입했으며 sheath를 통해 safety wire를 빈창자로 진행시켰다(Fig 2A). PJ catheter가 10mm Gooseneck Snare catheter (Medtronic, MN, USA)를 이용하여 단순 제거할 수 없는 위치에 있어 5Fr Contra catheter (Boston, MA ,US)를 삽입하고 Contra catheter 끝의 구부러진 부분을 silastic stent에 걸리도록 조작한 후 Terumo guidewire를 삽입하여 이자-빈창자 문합부 부근에서 wire loop를 만들었다 (Fig 2A, B) . Wire loop의 tip을 Gooseneck snare를 이용해 포획한 뒤 조심스럽게 14Fr sheath 바깥으로 꺼내고 7Fr Mc Namara sheath (Medtronic, MN, USA)를 넣어 stent가 걸려있는 wire loop snare의 끝을 조인 후 14Fr Sheath를 통해 제거하였다 (Fig 2C, D). 이후 시행한 담관 조영술에서 보인 담관석은 Fogarty balloon catheter를 통해 공장으로 밀어내고12Fr pig tail catheter를 삽입한 후 시술을 종료하였다.
추적관찰
익일 관 조영술을 시행하여 잔류 결석 및 췌담도 협착이 없음을 확인 후 경피경간 담도배액술 카테터를 제거하였고 환자는 안정적인 상태로 다른 합병증 없이 퇴원하였다. 3개월 이후 시행한 추적 복부 컴퓨터단층촬영에서도 담석은 보이지 않고 담관 확장 소견도 호전되었다.
Fig. 1.
Fig. 1. (A), (B), (C) Axial, coronal CT scan and PTBD tubogram showed PJ catheter inserted to pancreatic duct to prevent postoperative pancreatic juice leakage. The distal tip of catheter was migrated to left IHD.
Fig. 2.
Fig. 2. (A) A safety wire and 5F Cobra angiocatheter were inserted into jejunum via 14F sheath. (B). Another wire was inserted into jejunum through angiocatheter to make wire loop. Then distal wire loop was grabbed by gooseneck snare. (C), (D) The snared wire was then withdrawn through the sheath until both ends of the wire were outside the sheath
Fig. 3.
Fig. 3. On PTBD tubogram, a CBD stone was noted and pushed through hepatojejunostomy by using balloon catheter.
고찰
췌십이지장절제술 이후 췌공문합부 카테터의 이동은 흔하지 않지만 발생 시 췌장루, 간농양, 담관염, 담관의 협착, 담석 등의 다양한 합병증이 드물지 않게 나타날 수 있다 (5-8). Park 등의 보고에 따르면 802명의 췌십이지장절제술 및 췌공문합부 카테터 삽입을 시행한 환자 중에 16.8%가 담관 내로 카테터가 이동했으며 이 중 29.6%는 카테터로 유발된 합병증이 있었다 (5). Ogino 등은 CJ site에서 담관으로 이동된 카테터로 인해 담석이 유발된 증례를 보고하였다 (6). 이동된 스텐트가 머무는 기간과 합병증의 유의한 연관성을 보인다는 결과도 있어 신속한 회수가 시행되어야 한다 (5). 문합부 카테터 제거에 있어 내시경적 방법이 흔히 사용되어 왔으나 (3) 수술 후 해부학적 변화, 간내 담관으로의 카테터 이동, 간내 담석이 함께 동반된 경우에는 특히 경피경간 경로를 통한 카테터 및 담석 제거술이 유용한 해결책이다. 이동된 카테터 제거술에 대해 여러 증례와 소규모 연구들이 보고 되었으나, 표준화된 방법은 아직 정립되지 않았다. 담도로 이동되거나 매복되었던 여러 유형의 담도 내 기구를 스네어 및 생검 겸자등으로 제거한 보고들도 있었다 (3,10). 경피적 경간 경로를 통한 제거술은 한 세션으로 카테터와 담석의 동시 제거를 가능케 하여 유용하며, 간내 담관으로 카테터가 이동되어 카테터 끝을 snare 만으로 잡을 수 없는 경우 카테터 및 유도 철사를 이용해 이차적인 snare(secondary snare)를 형성하여 카테터를 제거하는 방법이 유용하며 안전한 치료 방법일 수 있다.
참고문헌
1. Roh YH, KH Kim, GJ Jung, YH Kim. Comparing the Results of Method of Jejunal Anastomosis at Pylorus�Preserving Pancreaticoduodenectomy. J Korean Surg Soc 2009; 77: 120-126.
2. Lu B, Cai X, Lu W, Huang Y, Jin X. Laparoscopic Pancreaticoduodenectomy to treat cancer of ampulla of vater. JSLS 2006;10:97-100
3. Koki N, Yasuaki A, Miyuki S, Norshazrima S, Minoru E, Kazuaki S. Successful Percutaneous Transhepatic Removal of an Internal Plastic Stent Migrated into the Intrahepatic Bile Duct after Pancreatoduodenectomy. Interventional Radiology 2017; 2: 19-24
4. Nanda V, Karthik D, Apoorva G, Sum L et al. Diagnosis and Management of Complications from Percutaneous Biliary Tract Interventions. Radiographics 2017;37:665-680
5. Park SH, Kim JH, Noh SY, Byun JH, Lee SS, Kim HJ, et al. Migration of internal pancreaticojejunostomy stents into the bile ducts in patients undergoing pancreatoduodenectomy. J Gastrointest Surg 2015; 19: 1995-2002.
6. Ogino M, Hirano S, Suzuki Y, Tanaka H, Saikawa D, Yamamoto K, et al. Biliary obstruction caused by stone formation around a long-term indwelling stent in choledochojejunostomy. Nihon Shokaki Geka Gakkai Zasshi 2015; 48: 840-846.
7. Kadowaki S, Miura F, Amano H, Toyota N, Wada K, Shibuya M, et al. Whereabouts of an internal short stent placed across the pancreaticojejunostomy following pancreatoduodenectomy. J Hepatobiliary Pancreat Sci 2012; 19: 566-577.
8. Gumus B. Percutaneous intervention strategies for the management of dysfunctioning biliary plastic endoprostheses in patients with malignant biliary obstruction. Diagn Interv Radiol 2012; 18:503?507.
9. Saad WE. Percutaneous transhepatic techniques for removal of endoscopically placed biliary plastic endoprostheses. Tech Vasc Interv Radiol 2008; 11:120?132.
10. Hsien-Tzu L, Hsiuo-Shan T, Nai-Chi C, Yi�Yang L, Yi-You C, Cien-An L. Percutaneous transhepatic techniques for retrieving fractured and intrahepatically dislodged percutaneous transhepatic biliary drainage catheters. Diagn Interv Radiol 2017; 23:461?464.
Citations
Citations to this article as recorded by