중심단어
Pseudoaneurysm, pancreaticoduodenal artery, celiac stenosis, coil embolization
국문 초록
61세 남자 환자가 3일간의 복통을 주소로 응급실에 내원하였다. 복부 CT에서 복강동맥 박리 및 혈전으로 인한 복강동맥 협착과 함께 췌십이지장동맥의 가성동맥류 및 주변 혈종이 관찰되었다. 이에 대한 진단 및 치료를 위해 응급 혈관조영술을 시행하였으며, 췌십이지장동맥에 두 개의 가성동맥류가 확인되었으며, 간혈류를 고려하여 하나의 가성동맥류만 코일 색전술을 시행하였다. 이후 시행한 복부 CT에서 가성동맥류 주변의 혈종은 흡수되었으며, 치료하지 않은 작은 가성동맥류의 크기도 감소하였다.
영문 초록
A 61-year-old man visited the emergency room with a 3-day history of abdominal pain. Abdominal CT identified two pseudoaneurysms at pancreaticoduodenal artery (PDA) with surrounding hematoma. Celiac stenosis by dissection and thrombus were also detected. A larger pseudoaneurysm was treated with coil embolization. On follow-up CT, hematoma around PDA was resolved and the size of untreated tiny aneurysm was decreased spontaneously.
Introduction
췌십이지장동맥(pancreaticoduodenal artery) 동맥류의 50-80%는 복강동맥 협착과 관련이 있다. 복강동맥 협착의 원인은 죽상경화증, 혈전, 선천성 무발생(결손) 및 정중활꼴인대에 인한 압박 등이 있다. 복강동맥 협착으로 인한 췌십이지장 동맥류의 주된 치료는 동맥류를 색전하는 것이며, 복강동맥 협착의 재개통에 대해서는 의견이 분분하다. 본 증례에서는 복강동맥 박리 및 혈전으로 인한 복강동맥의 협착으로 인해 췌십이지장동맥에 발생한 가성동맥류를 코일 색전술로 치료하였다.
Case report
증례
61세/남자
임상소견
61세 남자 환자는 3일간의 복부 통증으로 내원하였다. 혈액검사에서 고감도C반응성 단백이 약간 상승되어 있었으며(2.35 mg/dL) 그 외 특이 소견은 없었다. 환자의 기저력으로는 고혈압이 있으며, 왼쪽 상악동에 광범위큰B세포림프종으로 항암치료를 받아 완전관해 상태이다.
진단명
Pseudoaneurysms at pancreaticoduodenal arteries due to celiac stenosis
영상소견
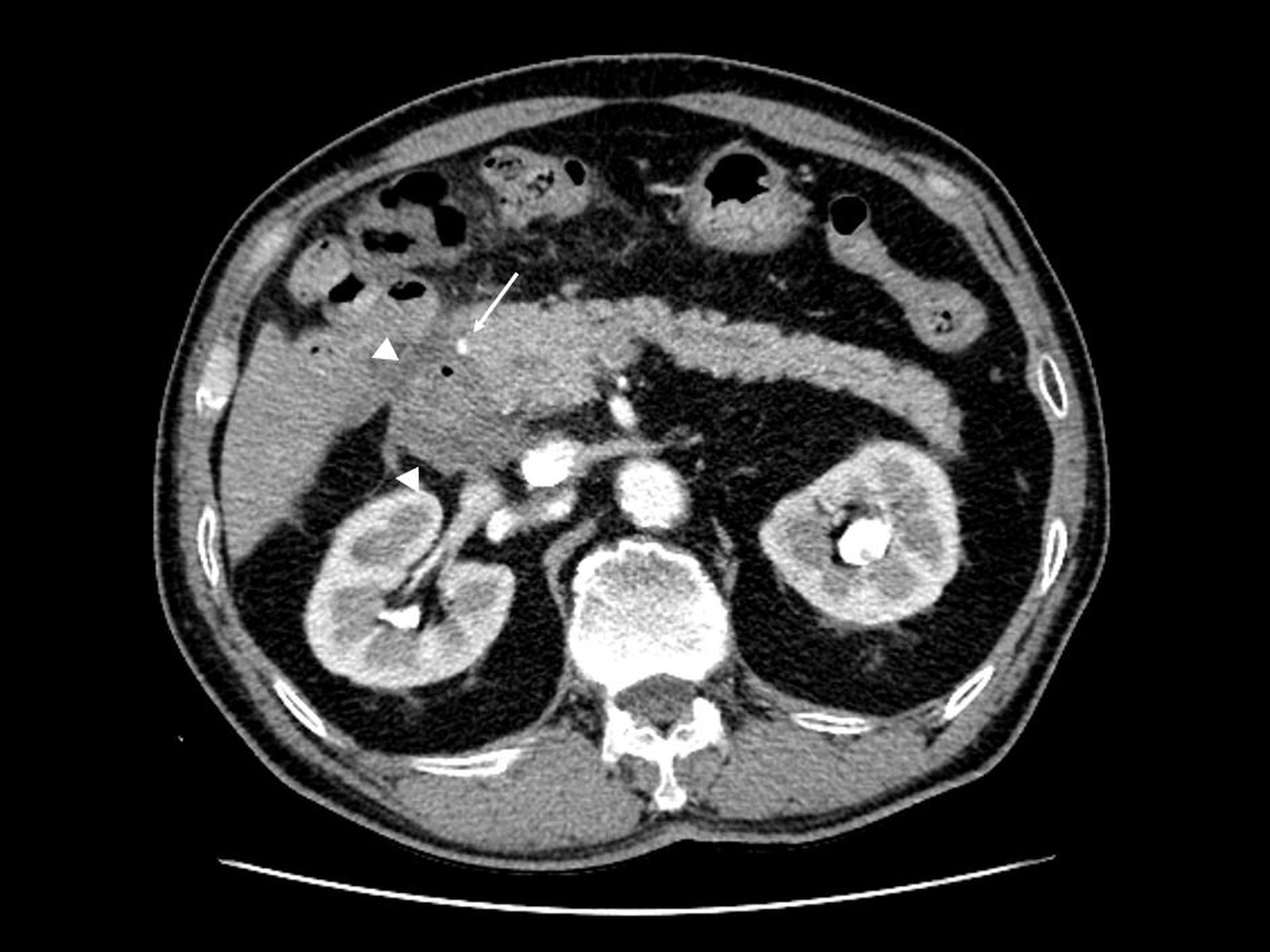
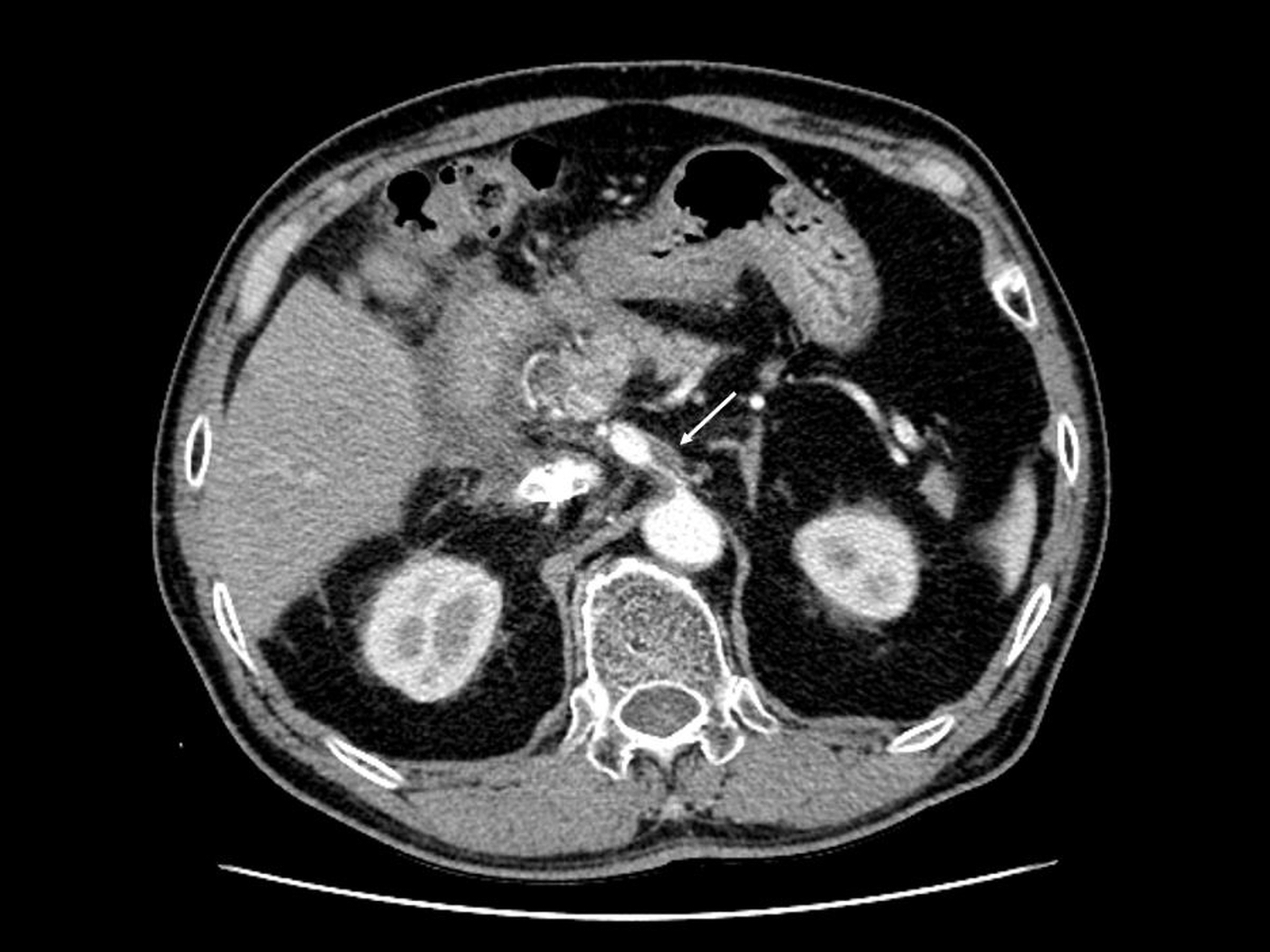
복부 CT에서 췌십이지장동맥의 앞가지(5mm)(Fig. 1A) 와 뒷가지(8mm)(Fig. 1B) 에 두 개의 가성동맥류가 있으며 주변으로 혈종이 관찰되었다. 그리고 복강동맥 박리로 인한 협착을 확인하였다(Fig. 1C).
시술방법 및 재료
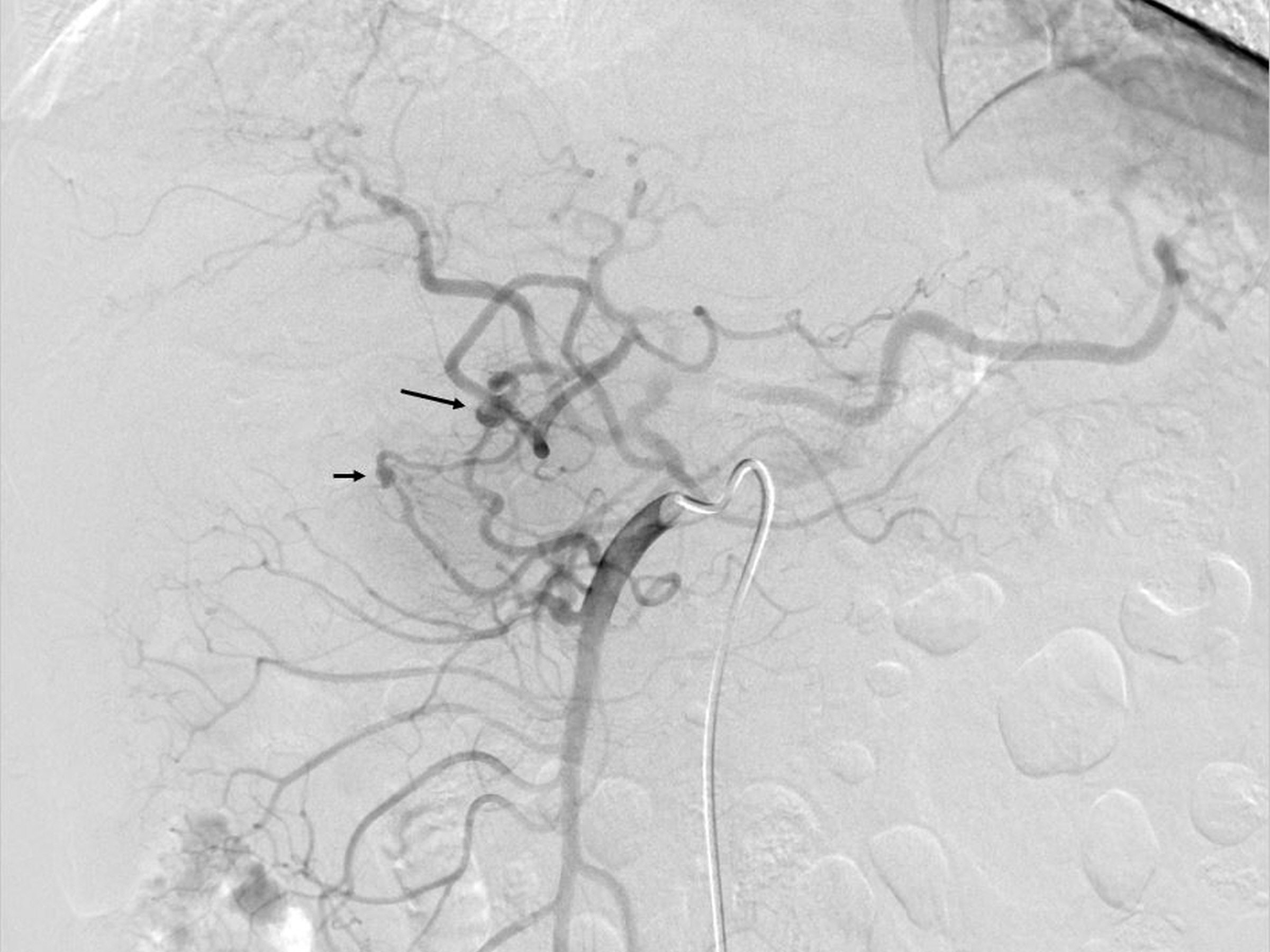
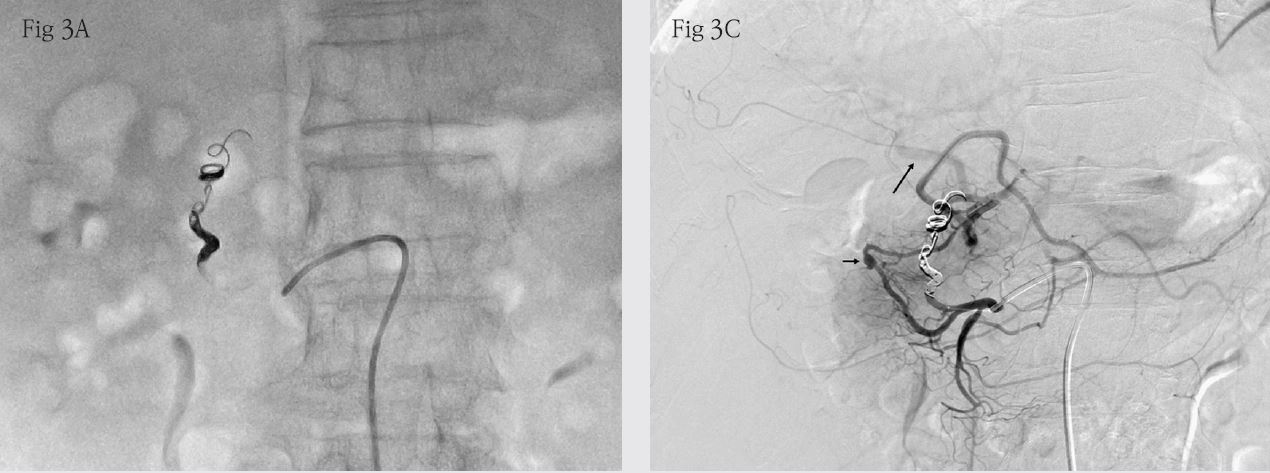
우측 대퇴동맥을 천자한 후 5Fr Simmons 1 catheter (A&A MD, Seongnam, Korea)를 이용하여 시행한 상장간막동맥 조영술에서 췌십이지장동맥에 두 개의 가성동맥류를 확인하였다(Fig. 2). 췌십이지장동맥 뒷가지를 1.9Fr microcatheter (Tellus, Asahi intecc, Aichi, Japan)로 선택한 후 가성동맥류의 앞뒤에 걸쳐 0.018” coil (6mm 1개, 4mm 1개, 3mm 1개; Nester embolization coil, Cook medical, Bloomington, IN, USA)을 이용하여 색전하였다(Fig 3A). 췌십이지장동맥 앞가지의 가성동맥류를 함께 색전할 경우 복강동맥 협착으로 인해 간으로 가는 혈류가 감소할 수 있어 이는 색전하지 않은 채 시술을 종료하였다.
추적관찰
환자는 시술 후 10일 뒤 추적 관찰을 위한 복부 CT를 시행하였으며, 가성동맥류 주변으로 보였던 hematoma가 대부분 흡수되었다. 췌십이지장동맥 앞가지의 가성동맥류(5mm)는 이후 크기 감소하여 약 3개월 후 CT에서는 명확하게 관찰되지 않았다.
Fig. 1. A
Fig. 1. Abdominal CT images show two pseudoaneurysms at (A) anterior (5mm) and (B) posterior (8mm) pancreaticoduodenal arteries with surrounding hematoma (arrowheads) as well as celiac stenosis by dissection and thrombus (C).
Fig. 1. B
Fig. 1. Abdominal CT images show two pseudoaneurysms at (A) anterior (5mm) and (B) posterior (8mm) pancreaticoduodenal arteries with surrounding hematoma (arrowheads) as well as celiac stenosis by dissection and thrombus (C).
Fig. 1. C
Fig. 1. Abdominal CT images show two pseudoaneurysms at (A) anterior (5mm) and (B) posterior (8mm) pancreaticoduodenal arteries with surrounding hematoma (arrowheads) as well as celiac stenosis by dissection and thrombus (C).
Fig. 2.
Fig. 2. Superior mesenteric arteriography illustrates two psuedoaneurysms at anterior (short arrow) and posterior (long arrow) pancreaticoduodenal arteries.
Fig. 3.
Fig. 3. A pseudoaneurysm of posterior branch is successfully treated with the coil embolization (A). A tiny pseudoaneurysm of anterior branch is left untreated (short arrow in B) and common hepatic arterial flow (long arrow) supplied by collateral from anterior pancreaticoduodenal artery is preserved.
고찰
복강 내 동맥류 중에 췌십이지장동맥의 동맥류 발생률은 1-2% 정도로 낮으며, 대부분은 비장동맥(60-80%), 간동맥(20%)에서 발생한다. 췌십이지장동맥 동맥류는 복강동맥의 협착 또는 폐색(50-80%)이 주된 원인이다. 복강동맥의 협착으로 인해 췌십이지장혈관궁(pancreaticoduodenal arcades)을 통해 대체 혈류를 공급받는 과정에서 췌십이지장동맥의 압력이 상승하고 혈관의 직경이 커지게 되어 동맥류가 유발되는 환경이 조성된다. 췌십이지장동맥 동맥류의 치료 가이드라인은 현재 명확히 정립되어 있지 않으나, 파열 가능성이 50%가 넘기 때문에 반드시 치료를 해야 한다고 보고되고 있다. 췌십이지장동맥 동맥류와 함께 복강동맥 협착이 같이 발견될 경우 동맥류의 원인으로 보이는 복강동맥 협착을 같이 치료를 하는 것에 있어서는 다소 의견이 분분하다. 최근에는 복강동맥의 재개통 없이 췌십이지장동맥 동맥류만 색전을 하였을 때 동맥류가 재발하지 않았다는 여러 연구결과가 나오고 있다. 본 케이스는 췌십이지장동맥 가성동맥류와 함께 복강동맥 박리로 인한 협착이 발견되었고, 복강동맥 협착으로 췌십이지장동맥 가성동맥류가 생겼을 것이라고 생각되지만 복강동맥 재개통에 대한 시술은 시도하지 않고, 췌십이지장동맥 가성동맥류만 색전을 하였으며 이후 경과 관찰에서 재발은 발견되지 않았다. 간혈류를 보전하기 위해 치료하지 않은 췌십이지장동맥 앞가지의 가성동맥류(5mm) 또한 그 크기가 감소하여 3개월 후 CT에서는 관찰되지 않았는데, 이는 복강동맥의 박리로 인한 협착이 호전되어 복강동맥을 통한 혈류량이 증가하면서 상대적으로 상장간막동맥을 통한 측부순환의 양이 감소하였기 때문인 것으로 생각된다.
참고문헌
1. Jesinger RA, Thoreson AA, Lamba R. Abdominal and pelvic aneurysms and pseudoaneurysms: imaging review with clinical, radiologic, and treatment correlation. Radiographics 2013;33:E71?E96
2. Murata S, Tajima H, Fukunaga T, Abe Y, Niggemann P, Onozawa S, et al. Management of pancreaticoduodenal artery aneurysms: results of superselective transcatheter embolization. AJR Am J Roentgenol 2006;187:W290-W298
3. Kalva SP, Athanasoulis CA, Greenfield AJ, Fan CM, Curvelo M, Waltman AC, et al. Inferior pancreaticoduodenal artery aneurysms in association with celiac axis stenosis or occlusion. Eur J Vasc Endovasc Surg 2007;33(6):670-675
4. Chivot C, Rebibo L, Robert B, Regimbeau JM, Yzet T. Ruptured pancreaticoduodenal artery aneurysms associated with celiac stenosis caused by the median arcuate ligament: a poorly known etiology of acute abdominal pain. Eur J Vasc Endovasc Surg 2016;51:295-301
5. Suzuki K, Tachi Y, Ito S, Maruyama K, Mori Y, Komada T, et al. Endovascular management of ruptured pancreaticoduodenal artery aneurysms associated with celiac axis stenosis. Cardiovasc Intervent Radiol 2008;31:1082?1087
6. Degheili JA, El Chediak A, Dergham MYR, Al-Kutoubi A, Hallal AH. Pancreaticoduodenal artery aneurysm associated with celiac trunk stenosis: case illustration and literature review. Case Rep Radiol 2017;6989673
Citations
Citations to this article as recorded by