중심단어
Portal vein, fistula, Stent-graft
국문 초록
췌장암으로 췌십이지장절제술을 받은 71세 여자 환자가 수술 후 3개월 추적관찰 복부 CT에서 주간문맥 폐색이 발견되어 인터벤션이 의뢰되었다. 문맥조영술에서 주간문맥 폐색 및 폐색부위에 문맥-소장루가 조영되었다. 문맥 폐색에 대해 스텐트 삽입 및 풍선확장술을 성공적으로 시행하였으나 시술 6일 후 스텐트 내에 조기 폐색이 발생하였고, 혈전 제거술 후 여전히 문맥-소장루가 조영되었다. 이에 대해서 스텐트 그라프트를 설치하였고 추적관찰에서 스텐트 그라프트가 잘 유지됨을 확인하였다.
영문 초록
A 71-year-old female patient who underwent pancreaticoduodenectomy for pancreatic cancer was followed-up for 3 months after the operation. An abdominal CT scan revealed an obliteration of main portal vein and vascular intervention was requested. Portography showed abrupt cutoff of main portal vein and portoenteric fistula was visualized at the occluded segment. Bare metal stent insertion and balloon angioplasty were successfully performed for portal vein obliteration. However, premature thrombotic stent occlusion occurred within the 6 days after the procedure. Aspiration thrombectomy and rheolytic thrombectomy was performed and portoenteric fistula was still noted at the stenting segment of portal vein. To resolve this, a stent graft was deployed in the previous bare metal stent. On the follow up CT, the stent graft was patent.
Introduction
췌장암은 의료기술이 발달한 현재에도 예후가 불량한 암으로, 완치를 위해서는 종양의 완전 절제가 필수적이지만 진단 당시 수술적 치료가 불가능한 병기로 발견되는 경우가 많다. 그러나 최근 전보조화학요법이나 방사선 치료가 췌장암에 적용됨에 따라 경계성 절제가능형 췌장암 (borderline resectable pancreatic cancer) 나 국소진행형 (locally advanced) 췌장암에서 주요 혈관 절제 및 재건과 함께 췌십이지장절제술을 시행하는 경우가 많아지고 있다 (1). 이로 인해 췌장수술 이후 문맥-장간막정맥 (portomesenteric vein)에 협착이나 폐색과 같은 합병증의 빈도가 증가할 것이라고 예상할 수 있고 (2), 수술 후 발생하 portomesenteric vein의 합병증에 스텐트 설치가 안전하고 효율적이라는 보고들이 있다 (3, 4). 저자들은 췌십이지장절제술과 혈관재건술을 함께 받은 환자에서 발생한 문맥-소장루 (portoenteric fistula)를 동반한 주간문맥혈전증을 스텐트 그라프트를 이용해 치료한 증례를 소개하고자 한다.
Case report
증례
71세/여자
임상소견
상장간막동맥과 상장간막정맥을 침범한 췌두부암 환자로 전보조화학요법과 체부정위 방사선치료 (Stereotactic ablative radiotherapy) 를 받은 후 췌십이지장절제술을 받았다. 수술할 때, 이전 방사선치료로 인한 유착이 심해 상장간막정맥-간문맥을 4cm가량 절제하고 bovine patch를 이용한 복원수술을 진행하였다. 수술 후 보조화학요법을 받으며 외래 추적관찰을 하였고, 수술 3개월 후 시행한 복부 CT에서 주간문맥 (main portal vein)의 폐색과 함께 다량의 복수가 확인되어 주간문맥에 대한 스텐트 시술이 의뢰되었다.
진단명
췌십이지장절제술 이후 발생한 간문맥 혈전증
영상소견
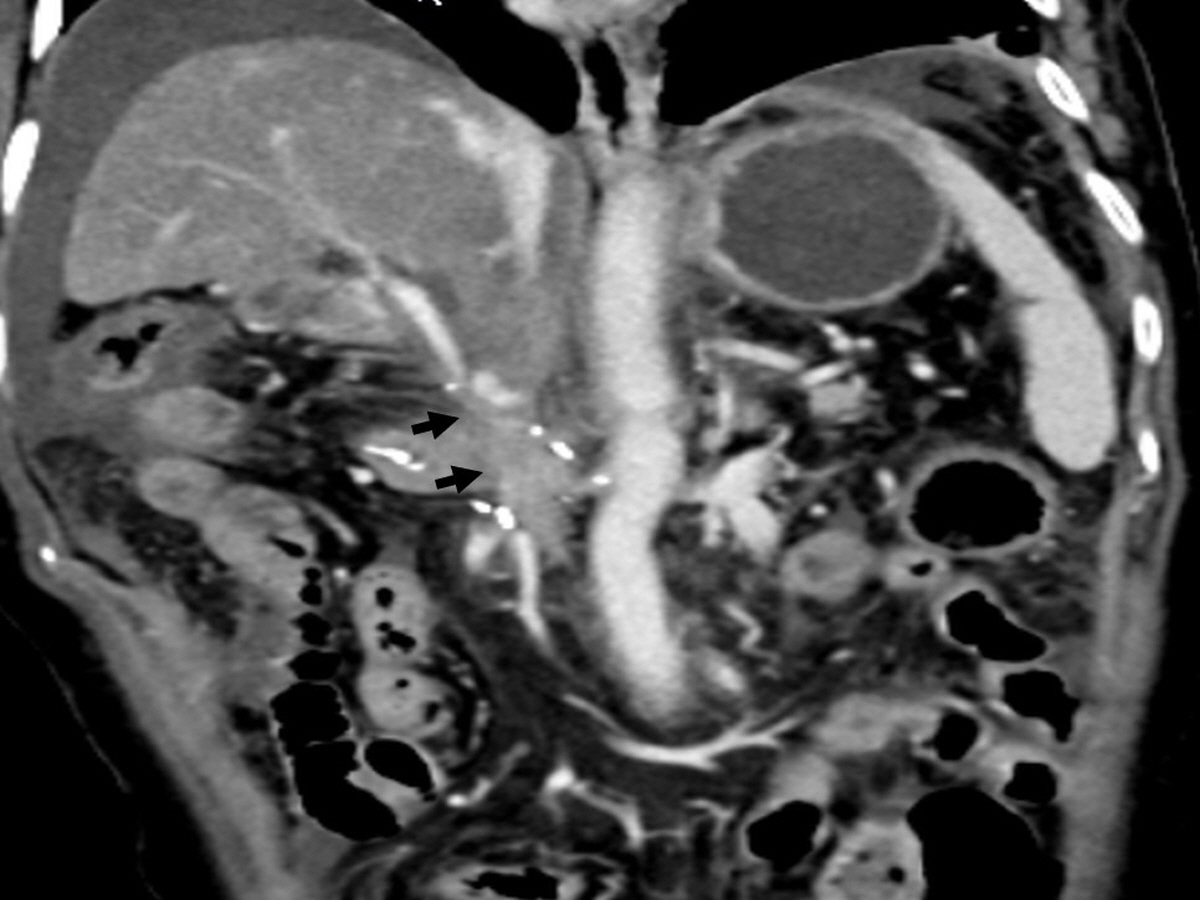
복부 CT에서 주간문맥의 폐색과 함께 다량의 복수가 있었다 (Fig. 1)
시술방법 및 재료
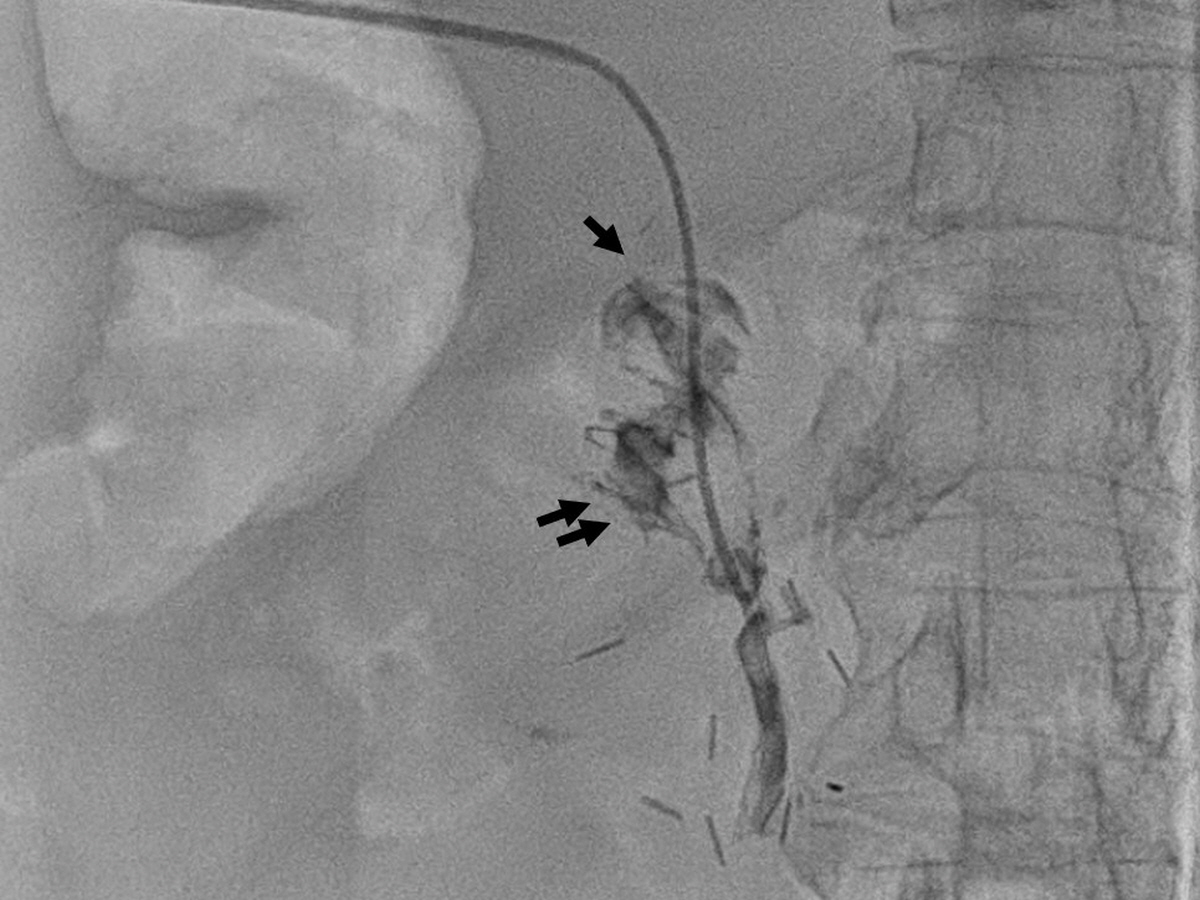
초음파 유도 하에 P5를 천자하여 5Fr sheath를 삽입하고 5Fr Davis catheter (Cook, Bloomington, IN, USA) 로 주간문맥에서 혈관조영술을 시행했을 때, 주간문맥의 급격한 폐색 소견이 관찰되었다 (Fig. 2A). 5Fr Davis catheter 와 0.035-inch, 150 cm long hydrophilic guide wire (Radiofocus Giude Wire M: Terumo, Tokyo, Japan) 를 이용하여 폐색된 간문맥 통과를 시도하였고, 폐색된 중간부위에서 조영제 주입 시 소장이 조영되었다 (Fig. 2B). 더 아래쪽으로 catheter 와 guidewire를 통과시켜 상장간막정맥 분지에서 혈관조영술을 시행하였을 때, 상장간막정맥 상방 간문맥쪽으로의 혈류는 없었으며 측부순환을 통한 혈류가 확인되었다 (Fig. 2C). 폐색된 주간문맥에 대해서 스텐트 (8mm x 6cm Zilver Flex Vascular Stent, Cook, Bloomington, IN, USA) 를 설치하고 풍선카테터 (6mm x 6cm, Mustang, Boston scientific, Marlborough, MA) 로 확장시켰다. 이후 상장간막정맥 분지에서 시행한 혈관조영술에서 간문맥으로의 혈류가 회복되고 측부순환이 소실된 것을 확인하였다 (Fig. 2D) 그러나 시술 4일째부터 혈액검사 소견 상 아미노전달효소 (AST, ALT) 수치가 상승하였고, 시술 6일 째 시행한 복부 CT 에서 간문맥 스텐트의 혈전성 폐색이 확인되어 다시 인터벤션이 의뢰되었다. 초음파 유도 하에 P5를 천자하여 7Fr sheath 를 삽입하고 0.035-inch wire 를 유지한 채 sheath 를 통해 문맥조영술을 시행하였고, 스텐트 내부에 혈전이 있음을 확인하였다 (Fig. 3A). 7Fr McNamara sheath (Cook, Bloomington, IN, USA) 로 수차례 흡인 혈전제거술 (aspiration thrombectomy) 을 하여 다량의 혈전을 제거하였으나 여전히 혈전이 일부 남아있어서 rheolytic thrombectomy 기구 (Angiojet Solent Proxi ,Boston Scientific, Maple Grove, Minnesota) 를 사용하여 혈전제거술을 시행하였다. 시술 중 조영제가 정체되는 상황에서 소장으로 조영제가 유입됨이 확인되었다 (Fig. 3B). 이후 5Fr Davis catheter를 상장간막정맥 분지에 위치시키고 시행한 문맥조영술에서 혈전은 상당부분 제거되었으나 여전히 스텐트 내부에 좁아보이는 부분이 있고, 일반 스텐트를 넣고 얼마 지나지 않아 폐색이 발생한 점을 고려하여 스텐트 그라프트 설치를 계획하였다. 7Fr sheath 를 8Fr sheath 로 교체한 후 스텐트 그라프트 (10mm x 6cm Covera Plus Vascular Covered Stent, BARD, Arizona, USA) 를 기존 스텐트 내부로 설치한 후, 풍선카테터 (8mm x 4cm, Mustang, Boston scientific, Marlborough, MA) 로 확장시켰다. 이후 시행한 문맥조영술에서 스텐트 내부의 협착 및 혈류가 호전됨을 확인하였다 (Fig. 3C)
추적관찰
6주 후 시행한 복부 CT 상 스텐트 그라프트의 개방성 (patency)이 잘 유지되고 있었으며, 10주 후 혈액검사에서 간 효소 수치는 정상이었다.
Fig. 1.
An multiplanar reformation image on portal venous phase shows segmental obliteration of main portal vein (arrows). Jejunal loop of hepatojejunostomy is adjacent to the obliterated portal vein.
Fig. 2.
(A) Portography with 5Fr Davis catheter shows abrupt cutoff of portal vein (arrow) (B) Obliterated portal vein is navigated with 5Fr Davis catheter and 0.035-inch wire. Contrast is injected at the mid portion of obliterated portal vein, and the smallbowel (arrows) is visualized suggesting an portoenteric fistula. (C) Superior mesenteric venography shows no blood flow toward the obliterated portal vein (arrow). Instead, blood flow through the collateral circulation is identified. Contrast in the small bowel lumen is observed. (D) Bare metal stent (arrow) is depolyed at the obliterated segment of portal vein and balloon dilatation is performed. Completion angiography shows restoration of blood flow to the portal vein and loss of collateral circulation.
Fig. 3.
(A) Portography through the 7Fr sheath shows thrombotic occlusion of portal vein. (B) After the thrombectomy, contrast is injected through the McNamara sheath and small bowel (arrow) was still visualized. (C) Stent graft is deployed (arrows) in the bare metal stent and dilatation was performed using balloon catheter. Completion angiography shows restoration of blood flow to the portal vein.
고찰
본 증례의 환자는 췌십이지장절제술 후 3개월만에 문맥 폐색이 발생하였고 문맥조영술 상 문맥과 소장 사이의 누공이 있었으며, 여기에 스텐트를 설치하였으나 일주일만에 스텐트의 조기 폐색이 발생하였다. 이후 스텐트 내부에서 시행한 문맥조영술에서도 소장과의 누공이 확인되었고, 스텐트 그라프트를 사용하여 소장 내용물의 문맥 혈류로의 유입을 차단한 이후로는 문맥의 개방성이 추적관찰 기간동안 잘 유지되었다. 이는 경경정맥간내문맥정맥단락술 (Transjugular intrahepatic portosystemic shunt, TIPS) 의 간실질내 부분에서의 조기 폐색이 담도루 (biliary fistula) 와 연관이 있으며 스텐트 그라프트를 사용하여 담즙의 혈류로의 유입을 차단함으로써 성공적으로 개방성을 유지하였다는 이전 보고들과 맥락을 같이 한다 (5-7). 따라서 췌담도수술 후 주변 체액의 혈관내로의 유출이 의심 혹은 확인된 문맥협착이나 폐색에서는 본 증례와 같이 스텐트 그라프트를 치료 옵션으로 생각해 볼 수 있겠다.
참고문헌
1. Croome KP, Farnell MB, Que FG, Reid�Lombardo KM, Truty MJ, Nagorney DM, et al. Pancreaticoduodenectomy with major vascular resection: a comparison of laparoscopic versus open approaches. J Gastrointest Surg 2015;19:189-194; discussion 194
2. Gao W, Dai X, Dai C, Jiang K, Wu J, Li Q, et al. Comparison of patency rates and clinical impact of different reconstruction methods following portal/superior mesenteric vein resection during pancreatectomy. Pancreatology 2016;16:1113-1123
3. Zhou ZQ, Lee JH, Song KB, Hwang JW, Kim SC, Lee YJ, et al. Clinical usefulness of portal venous stent in hepatobiliary pancreatic cancers. ANZ J Surg 2014;84:346-352
4. Jeon UB, Kim CW, Kim TU, Choo KS, Jang JY, Nam KJ, et al. Therapeutic efficacy and stent patency of transhepatic portal vein stenting after surgery. World J Gastroenterol 2016;22:9822-9828
5. Saxon RR, Mendel-Hartvig J, Corless CL, Rabkin J, Uchida BT, Nishimine K, et al. Bile duct injury as a major cause of stenosis and occlusion in transjugular intrahepatic portosystemic shunts: comparative histopathologic analysis in humans and swine. J Vasc Interv Radiol 1996;7:487-497
6. Sze DY, Vestring T, Liddell RP, Kato N, Semba CP, Razavi MK, et al. Recurrent TIPS failure associated with biliary fistulae: treatment with PTFE-covered stents. Cardiovasc Intervent Radiol 1999;22:298-304
7. Suhocki PV, Smith AD, Tendler DA, Sexton DJ. Treatment of TIPS/biliary fistula-related endotipsitis with a covered stent. J Vasc Interv Radiol 2008;19:937-939
Citations
Citations to this article as recorded by