중심단어
Hepatocellular carcinoma, Transarterial radioembolization (TARE), hepatic artery
국문 초록
만성 B형 간염이 있는 66세 여자환자가 새롭게 발견된 간세포암에 대해 방사선 색전술을 받기 위해 내원하였다. 시술 도중 간동맥 혈전증이 발생하였고, tPA 를 사용하여 카테터 유도 혈전용해술을 시행한 후 치료를 완료하였다. 추적관찰에서 간세포암의 관해가 확인되었다.
영문 초록
A 66-year-old female patient with chronic hepatitis B was admitted for transarterial radioembolization for newly diagnosed hepatocellular carcinoma. Hepatic artery thrombosis occurred during the procedure, and the treatment was completed after catheter�directed thrombolysis using tPA. Remission of hepatocellular carcinoma was confirmed at follow-up.
Introduction
방사선색전술 (Transarterial radioembolization, TARE)은 이트륨 90 (yttrium 90, Y-90) 을 탑재한 미세구 (microsphere) 를 간동맥내로 주입하여 간세포암을 치료하는 시술이다. 경동맥화학색전술 (Transarterial chemoembolization, TACE) 과 비교했을 때, 생존률에 큰 차이는 없으나 경동맥화학색전술에 비해 time-to-progression (TTP) 이 길고, 색전후증후군이 적으며, 재원기간이 짧다는 장점이 있어 간세포암의 치료에 많이 이용되고 있다 (1, 2). 한편 경동맥화학색전술과 연관되어 생길 수 있는 여러 합병증 중 catheter 나 guidewire의 조작과정에서 간동맥의 연축 (spasm), 박리 (dissection), 혈전증 (thrombosis) 등이 생길 수 있고, 이러한 경우 종양으로 가는 혈류의 장애를 일으켜 적절한 치료를 방해할 수도 있다 (3, 4). 저자들은 방사선색전술 시술 도중 발생한 간동맥 혈전을 해결하고 성공적으로 방사선색전술을 시행하였던 증례를 보고하고자 한다.
Case report
증례
66세/여자
임상소견
만성 B형 간염으로 정기 검진 중 새롭게 발견한 간세포암에 대한 치료를 위해서 내원하였다.
진단명
간세포암 (hepatocellular carcinoma)
영상소견
복부 CT에서 간의 7번 분절과 8번 분절에 걸쳐 장경 8cm 가량의 간세포암이 있고, 그 주변으로 작은 위성 결절들이 의심되었다 (Fig. 1). 방사선색전술의 가능여부를 확인하기 위해 우간동맥에 Tc-99m MAA 를 주입하여 lung shunt scan 을 시행하였고, lung shunt fraction 2.93% 로 방사선색전술에 적합하였다.
시술방법 및 재료
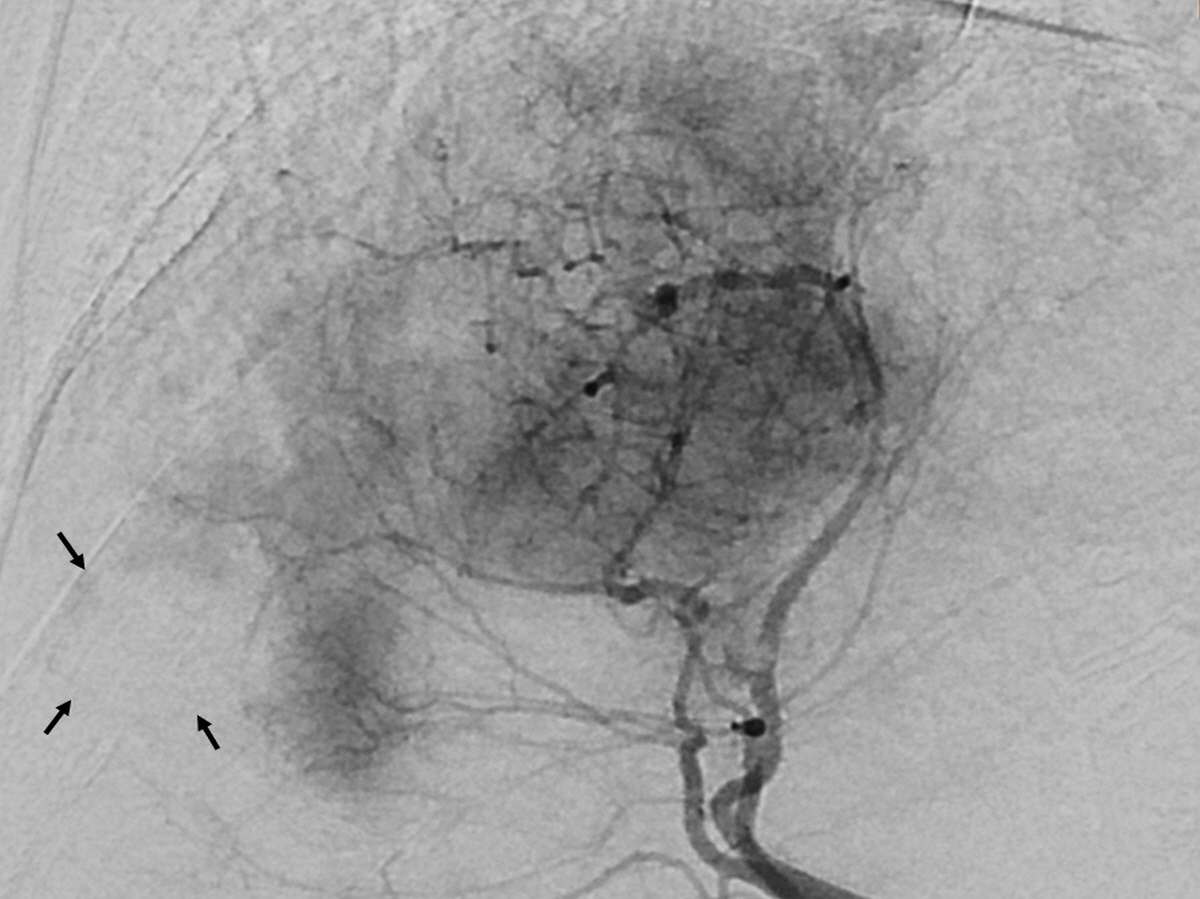
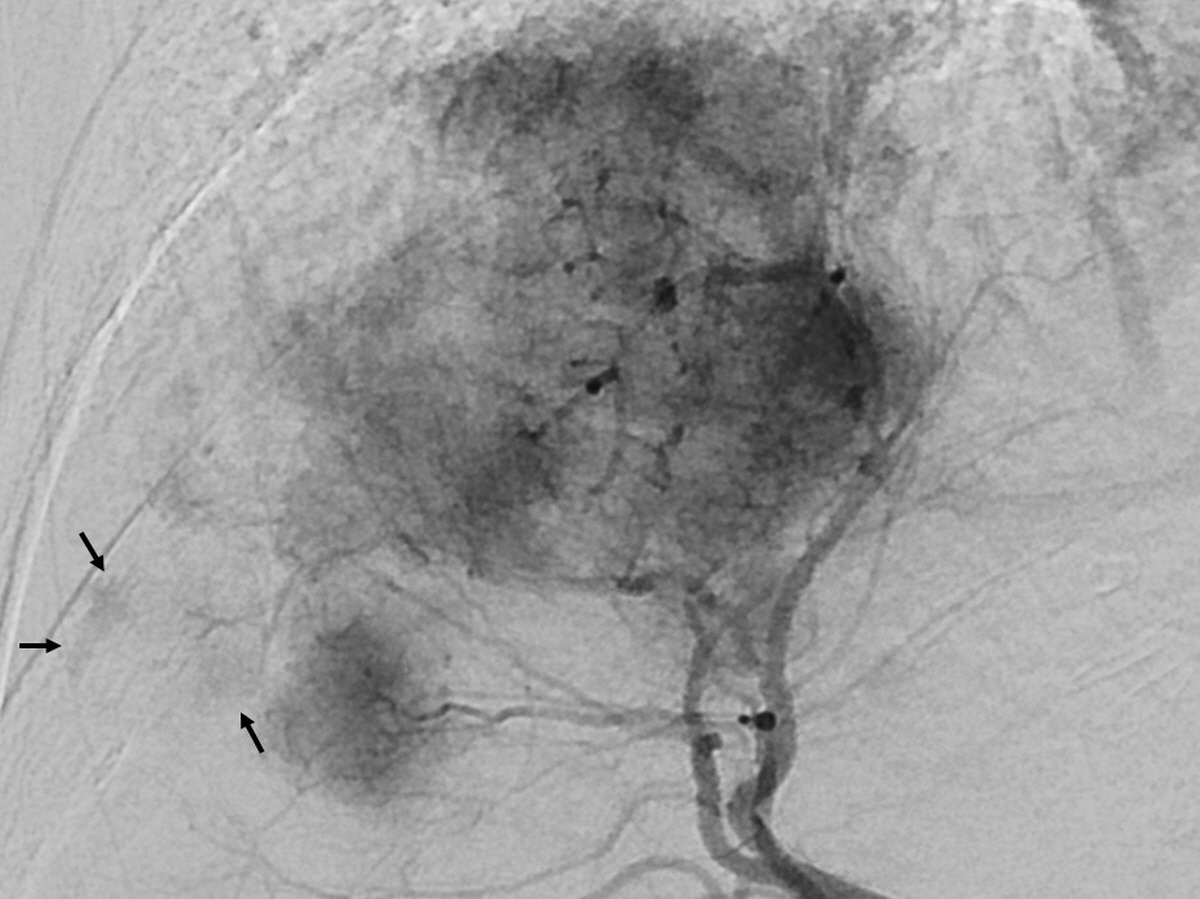
초음파 유도 하에 우측 대퇴동맥을 천자하여 5Fr sheath를 삽입 후, 5Fr RH catheter (Cook, Bloomington, IN, USA)를 총간동맥에 위치키시고 혈관조영검사를 시행하여 종양의staining을 확인하였다 (Fig. 2A). 종양이 dome 쪽에 위치하고 있어 측부순환에 의한 혈액공급을 받을 가능성이 있기 때문에, 이를 확인하기 위해 우측 하횡격막동맥조영술을 계획하고 RH catheter를 복강동맥 입구에 위치시켰다. 이후, Carnelian 1.8 microcatheter (Tokai Medical, Gifu, Japan) 와 0.014-inch TransendTM guidewire (Boston scientific, Natick, MA) 로 우측 하횡격막동맥 선택을 시도하였다. 그러나 우측 하횡격막동맥이 복강동맥 근위부에서 기시하여 선택적 조영술을 하기까지 시간이 오래 걸렸으며, 그 과정에서 microcatheter 와 guidewire 가 반복적으로 RH catheter 내부를 지나게 되었다. 우측 하횡격막동맥에 대한 선택적 조영술에서 종양 staining 은 확인되지 않았다 (Fig. 2B). 종양에 혈액을 공급하는 5번 분절과 8번 분절의 간동맥에 대해 TheraSphere® glass microspheres (BTG, London, United Kingdom) 로 방사선색전술을 계획하고, TheraSphere 를 주입하기 전 8번 분절 간동맥에서 조영술을 시행하였다. 처음에는 보이지 않던 혈관 내 filling defect 가 보였고, 종양 staining 도 일부 보이지 않았다 (Fig. 2C, 2D). 시술 도중 발생한 간동맥 내 혈전을 없애기 위해 해당 동맥 분지에 대해 tPA 3mg, nitroglycerin 300μg을 일시주사 (bolus injection) 하였고, 이후 시행한 혈관조영술에서 혈전의 범위가 감소한 것을 확인 후 방사선색전술을 시행하였다 (Fig. 2E)
추적관찰
추적관찰을 위해 정기적으로 복부 CT를 촬영하였고, 방사선색전술 1년 후 검사에서도 간세포암의 재발 없이 완전관해를 유지하였다. (Fig. 3)
Fig. 1.
An arterial phase CT image shows a 8cm sized hepatocellullar carcinoma in the segment 7/8 of the liver.
Fig. 2.
(A) A common hepatic arteriogram with 5Fr RH catheter shows a hypervascular tumor staining in the right lobe of the liver. Tumor is supplied by the segment 5 hepatic artery and segment 8 hepatic artery. (B) A right inferior phrenic arteriogram with 1.7Fr microcatheter shows no tumor staining. (C), (D) On the right anterior hepatic arteriogram, there are filling defects (white arrows) suggesting thrombosis in the segment 8 hepatic artery branches. Also, some ofthe tumor staining (black arrow) is not visible. (E) After administration of 3mg of tPA and 300μg of nitroglycerin through the microcatheter, the extent of thrombus in segment 8 hepatic artery branches decreased, and some of the invisible tumor staining recovered (arrow).
Fig. 3.
On follow-up CT after 1 year of TARE, there is no evidence of viable hepatocellular carcinoma, only dystrophic calcifications remain.
고찰
간세포암 환자에 대한 경동맥 (transarterial) 치료는 수술적 절제가 불가능한 환자에서 효과적인 치료법이나, 동맥 내에서 catheter나 guidewire를 조작하는 과정에서 동맥의 연축이나 박리, 혈전증과 같은 합병증을 유발할 수 있다 (3, 4). 본 증례의 경우 간세포암의 측부순환에 의한 혈류 공급을 확인하기 위해 하횡격막동맥을 microcatheter와 guidewire로 선택하는 과정에서 선택이 어려워 RH catheter 내부로 여러 번 microcatheter와 guidewire가 드나들면서, 긴 시간동안 RH catheter 내에 만들어져 있던 혈전이 간동맥 내부로 이동하면서 간동맥 혈전증이 유발되었을 것으로 생각된다. Tissue plasminogen activator (tPA) 는 혈관 내피 (endothelium) 에서 유래된 물질로 DNA 기술을 이용하여 인공적으로 만든 recombinant tissue plasminogen activator (rtPA) 로서 사용된다. 이는 직접적인 plasminogen activator 로 normal circulation 에서는 상대적으로 불활성화 상태로 있다가 thrombus 의 fibrin 과 결합하면 plasminogen 을 plasmin 으로 변형시켜서 혈전을 용해시킬 수 있게 한다. 따라서 다른 전신 IV 주사 혈전용해제와는 다르게 혈전이 있는 부위에 직접 투여하여 국소부위의 rtPA 농도를 높임으로써 치료효과를 더 높일 수 있게 사용하고 있으며, 급성사지허혈증의 catheter를 이용한 혈전용해술에서 널리 사용되고 있다 (5). 본 증례에서도 급성으로 발생한 간동맥혈전에 tPA를 사용하여 혈전을 용해시켜 혈류를 개통시킴으로써 방사선 색전물질이 종양 혈관내로 효과적으로 전달될 수 있게 하였다. 환자에 대한 치료를 하는 과정에서 합병증이 발생하지 않도록 예방하는 것이 가장 좋은 방법이겠지만, 본 증례는 의도치 않게 발생한 합병증에 대해 최선의 해결방법을 이용하여 좋은 결과를 얻을 수 있었던 사례였다.
참고문헌
1. Moreno-Luna LE, Yang JD, Sanchez W, Paz�Fumagalli R, Harnois DM, Mettler TA, et al. Efficacy and safety of transarterial radioembolization versus chemoembolization in patients with hepatocellular carcinoma. Cardiovasc Intervent Radiol 2013;36:714-723
2. Kallini JR, Gabr A, Salem R, Lewandowski RJ. Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma. Adv Ther 2016;33:699-714
3. Yoon DY, Park JH, Chung JW, Han JK, Han MC. Iatrogenic dissection of the celiac artery and its branches during transcatheter arterial embolization for hepatocellular carcinoma: outcome in 40 patients. Cardiovasc Intervent Radiol 1995;18:16-19
4. Clark TW. Complications of hepatic chemo embolization. Semin Intervent Radiol 2006;23:119-125
5. Morrison HL. Catheter-directed thrombolysis for acute limb ischemia. Semin Intervent Radiol 2006;23:258-269
Citations
Citations to this article as recorded by